A brain arteriovenous malformation (AVM) is a tangle of blood vessels that connects arteries and veins in the brain.
The arteries take oxygen-rich blood from the heart to the brain. Veins carry the oxygen-depleted blood back to the lungs and heart. A brain AVM disrupts this vital process.
An arteriovenous malformation can develop anywhere in the body but common locations include the brain and spinal cord — though overall, brain AVMs are rare.
The cause of brain AVMs isn't clear. Most people are born with them, but they can form later in life. Rarely, they can be passed down among families.
Some people with a brain AVM experience signs and symptoms, such as headaches or seizures. An AVM is often found after a brain scan for another health issue or after the blood vessels rupture and bleed (hemorrhage).
Once diagnosed, a brain AVM can be treated to prevent complications, such as brain damage or stroke.
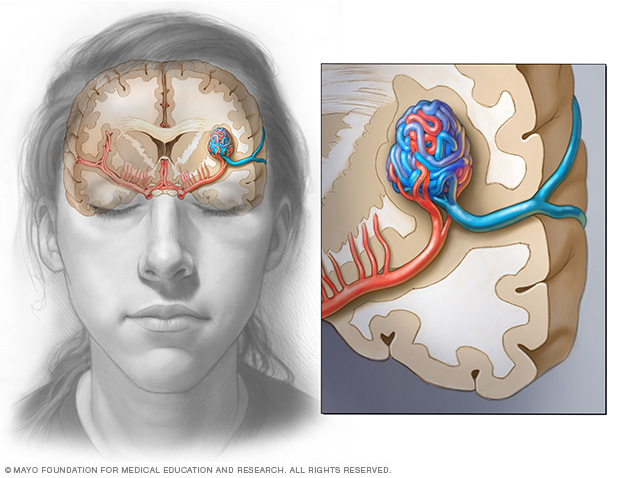
In a brain AVM, blood passes directly from the arteries to the veins via tangled vessels. This disrupts the typical process of how blood circulates through the brain.
In a brain arteriovenous malformation, blood passes directly from arteries to veins through a tangle of blood vessels.
Symptoms
A brain arteriovenous malformation may not cause any signs or symptoms until the AVM ruptures, resulting in hemorrhage. In about half of all brain AVMs, hemorrhage is the first sign.
But some people with brain AVM may experience signs and symptoms other than bleeding, such as:
- Seizures
- Headache or pain in one area of the head
- Muscle weakness or numbness in one part of the body
Some people may experience more-serious neurological signs and symptoms, depending on the location of the AVM, including:
- Severe headache
- Weakness, numbness or paralysis
- Vision loss
- Difficulty speaking
- Confusion or inability to understand others
- Severe unsteadiness
Signs and symptoms of a brain AVM may begin at any age but usually emerge between ages 10 and 40. Brain AVMs can damage brain tissue over time. The effects slowly build and often cause symptoms in early adulthood.
By middle age, however, brain AVMs tend to remain stable and are less likely to cause symptoms.
Research hasn't found that pregnancy increases the risk of hemorrhage for people with a brain AVM. However, more research needs to be done.
One severe type of brain AVM involves the vein of Galen. It causes signs and symptoms that emerge soon or immediately after birth. The major blood vessel involved in this type of brain AVM can cause fluid to build up in the brain and the head to swell. It can also cause swollen veins that are visible on the scalp, seizures, failure to thrive and congestive heart failure.
When to see a doctor
Seek immediate medical attention if you notice any signs or symptoms of a brain AVM, such as seizures, headaches or other symptoms. A bleeding brain AVM is life-threatening and requires emergency medical attention.
Causes
The cause of brain AVM is unknown. Researchers believe most brain AVMs are present at birth and form during fetal development, but brain AVMs can develop later in life, as well. Brain AVMs are seen in some people who have hereditary hemorrhagic telangiectasia (HHT), also known as Osler-Weber-Rendu syndrome. HHT affects the way blood vessels form in several areas of the body, including the brain.
Typically, the heart sends oxygen-rich blood to the brain through arteries. The arteries slow blood flow by passing it through a series of progressively smaller networks of blood vessels, ending with the smallest blood vessels (capillaries). The capillaries slowly deliver oxygen through their thin, porous walls to the surrounding brain tissue.
The oxygen-depleted blood passes into small blood vessels and then into larger veins that return the blood to the heart and lungs to get more oxygen.
The arteries and veins in an AVM lack this supporting network of smaller blood vessels and capillaries. Instead, blood flows quickly and directly from the arteries to the veins, bypassing the surrounding tissues.
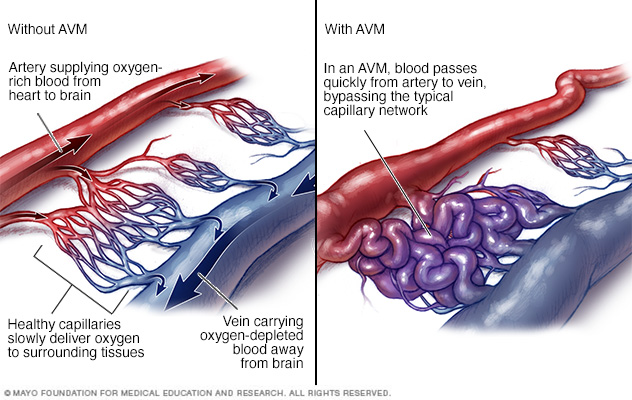
In an arteriovenous malformation (AVM), blood passes quickly from the arteries to the veins, disrupting the typical blood flow and depriving the surrounding tissues of oxygen.
Risk factors
Anyone can be born with a brain AVM, but these factors may raise the risk:
- Being male. Brain AVMs are more common in males.
- Having a family history. In rare cases, brain AVMs have been reported to occur in families, but it's unclear if there's a certain genetic factor or if the cases are only coincidental. It's also possible to inherit other medical conditions that increase the risk of brain AVMs, such as hereditary hemorrhagic telangiectasia (HHT).
Complications
Complications of a brain AVM include:
-
Bleeding in the brain. An AVM puts extreme pressure on the walls of the affected arteries and veins, causing them to become thin or weak. This may result in the AVM rupturing and bleeding into the brain.
This risk of a brain AVM bleeding ranges from around 2% to 3% each year. The risk of bleeding may be higher for certain types of AVMs or if there's been a previous AVM rupture.
Some hemorrhages associated with AVMs go undetected because they cause no major brain damage or signs or symptoms. However, potentially life-threatening bleeding episodes may occur.
Brain AVMs account for about 2% of all hemorrhagic strokes each year. They're often the cause of hemorrhage in children and young adults who experience brain hemorrhage.
-
Reduced oxygen to brain tissue. With a brain AVM, blood bypasses the network of capillaries and flows directly from arteries to veins. Blood rushes quickly through the altered path because it isn't slowed by channels of smaller blood vessels.
Surrounding brain tissue can't easily absorb oxygen from the fast-flowing blood. Without enough oxygen, brain tissues weaken or may die off completely. This results in stroke-like symptoms, such as difficulty speaking, weakness, numbness, vision loss or severe unsteadiness.
- Thin or weak blood vessels. An AVM puts extreme pressure on the thin and weak walls of the blood vessels. A bulge in a blood vessel wall (aneurysm) may develop and become susceptible to rupture.
-
Brain damage. The body may recruit more arteries to supply blood to the fast-flowing brain AVM. As a result, some AVMs may get bigger and displace or compress portions of the brain. This may prevent protective fluids from flowing freely around the hemispheres of the brain.
If fluid builds up, it can push brain tissue up against the skull.
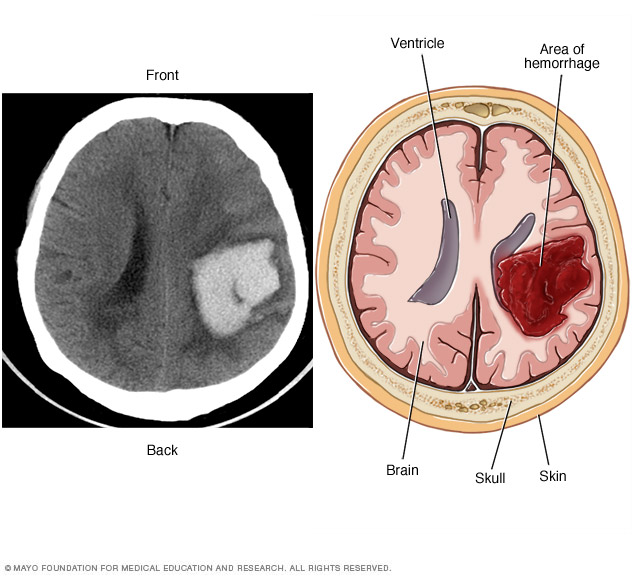
A brain AVM may cause bleeding in the brain (hemorrhage), which can damage the surrounding brain tissue, as shown by this CT scan (left) and illustration (right) of an intracerebral hemorrhage.
Diagnosis
To diagnose a brain AVM, your health care provider will review your symptoms and conduct a physical exam.
One or more tests may be used to diagnose brain AVM. Radiologists trained in brain and nervous system imaging (neuroradiologists) usually conduct imaging tests.
Tests used to diagnose brain AVMs include:
-
Cerebral angiography. Also known as cerebral arteriography, this is the most detailed test to diagnose a brain AVM. Cerebral angiography reveals the location and characteristics of the feeding arteries and draining veins, which is critical to planning treatment.
In this test, a long, thin tube (catheter) is inserted into an artery in the groin or wrist and is threaded to the brain using X-ray imaging. A dye is injected into the blood vessels of the brain to make them visible under X-ray imaging.
-
Computerized tomography (CT) scan. A CT scan uses a series of X-rays to create a detailed cross-sectional image of the brain.
Sometimes a dye is injected through a tube into a vein for the CT scan (computerized tomography angiography). The dye allows the arteries feeding the AVM and the veins draining the AVM to be viewed in greater detail.
-
Magnetic resonance imaging (MRI). MRI uses powerful magnets and radio waves to create detailed images of the brain.
MRI is more sensitive than CT and can show more subtle changes in brain tissue associated with a brain AVM.
MRI also provides information about the exact location of the brain AVM and any related bleeding in the brain, which is important for determining treatment options.
A dye may also be injected to see the blood circulation in the brain (magnetic resonance angiography.
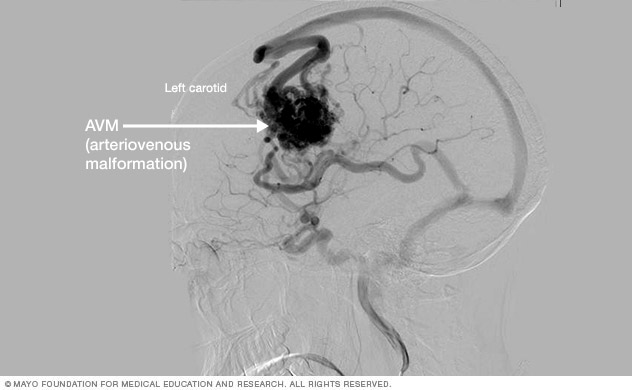
Cerebral angiogram showing brain AVM
A CT scan can be used to visualize nearly all parts of the body and is used to diagnose disease or injury as well as to plan medical, surgical or radiation treatment.

Treatment
There are several potential treatment options for brain AVM. The main goal of treatment is to prevent hemorrhage, but treatment to control seizures or other neurological complications also may be considered.
The most appropriate treatment for your condition depends on your age, health, and the size and location of the brain AVM.
Medications may be used to treat symptoms caused by the AVM, such as headaches or seizures.
Surgery is the most common treatment for brain AVMs. There are three surgical options:
-
Surgical removal (resection). If the brain AVM has bled or is in an area that can easily be reached, brain surgery to remove the AVM may be recommended. In this procedure, the surgeon removes part of the skull temporarily to gain access to the AVM.
With the help of a high-powered microscope, the surgeon seals off the AVM with special clips and carefully removes it from surrounding brain tissue. The surgeon then reattaches the skull bone and closes the incision in the scalp.
Resection is usually done when the AVM can be removed with little risk of hemorrhage or seizures. AVMs that are in deep brain regions carry a higher risk of complications. In these cases, your health care provider may recommend other treatments.
-
Endovascular embolization. In this procedure, a catheter is inserted into an artery in the leg or wrist and is threaded through blood vessels to the brain using X-ray imaging.
The catheter is positioned in one of the arteries that feeds the brain AVM. The surgeon injects an embolizing agent — such as small particles, a glue-like substance, microcoils or other materials — to block the artery and reduce blood flow into the AVM.
Endovascular embolization is less invasive than traditional surgery. It may be performed alone. But it is frequently used prior to other surgical treatments to make them safer. It does this by reducing the size of the brain AVM or the likelihood of bleeding.
In some large brain AVMs, endovascular embolization may be used to reduce stroke-like symptoms by redirecting blood back to brain tissue.
-
Stereotactic radiosurgery (SRS). This treatment uses precisely focused radiation to destroy the AVM. It isn't surgery in the literal sense because there is no cuts into the body.
Instead, SRS directs many highly targeted radiation beams at the AVM to damage the blood vessels and cause scarring. The scarred AVM blood vessels then slowly clot off in 1 to 3 years following treatment.
This treatment is most appropriate for small AVMs that are difficult to remove with conventional surgery and for those that haven't caused a life-threatening hemorrhage.
If you have few or no symptoms or if your AVM is in an area of your brain that's hard to treat, your health care provider may decide to monitor your condition with regular checkups.
Potential future treatments
Researchers are currently studying ways to better predict the risk of hemorrhage in people with brain AVM to better guide treatment decisions. For example, high blood pressure within the AVM and hereditary syndromes associated with neurological issues may play a role.
Innovations in imaging technology — such as 3D imaging, brain tract mapping and functional imaging, which produces images of blood flow to certain areas of the brain — also are being evaluated. The techniques have the potential to improve surgical precision and safety in removing brain AVMs and preserving surrounding vessels.
In addition, ongoing advances in embolization, radiosurgery and microsurgery techniques are making previously inoperable brain AVMs more accessible and safer for surgical removal.
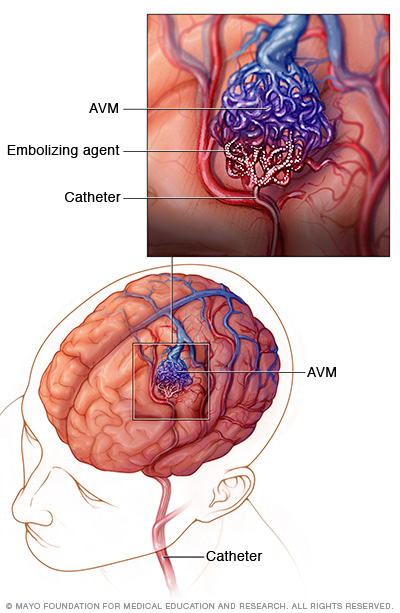
In endovascular embolization, a long, thin tube (catheter) is inserted into a leg artery and is threaded through blood vessels to the brain using X-ray imaging. The surgeon positions the catheter in one of the arteries that feeds the AVM and injects an embolizing agent, such as small particles or a glue-like substance, to block the artery and reduce blood flow into the AVM.
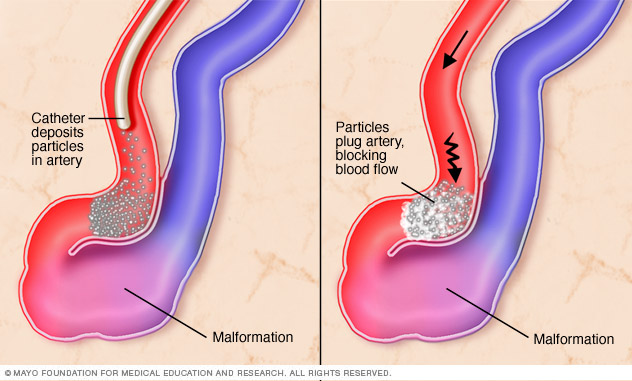
In endovascular embolization for AVM, a catheter deposits particles of a gluelike substance in the affected artery to block blood flow.
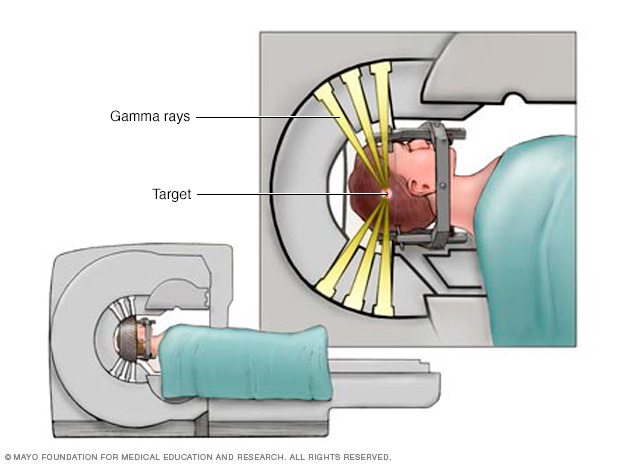
Individual radiation beams are too weak to hurt the brain tissue they travel through on the way to the target. The radiation is most powerful where all the beams intersect.
Coping and support
You can take steps to cope with the emotions that may come with a diagnosis of brain AVM and the recovery process. Consider trying to:
- Learn about brain AVM to make informed decisions about your care. Ask your health care provider about the size and location of your brain AVM and how that affects your treatment options. As you learn more about brain AVMs, you may become more confident in making treatment decisions.
- Accept your emotions. Complications of brain AVM, such as hemorrhage and stroke, can cause emotional issues as well as physical ones. Recognize that experiencing the emotions is common. Some emotional and mood changes may be caused by the injury itself, along with coming to terms with the diagnosis.
- Keep friends and family close. Keeping your close relationships strong will help you during your recovery. Friends and family can provide the practical support you'll need, such as coming with you to health care appointments and providing emotional support.
- Find someone to talk with. Find a good listener who is willing to listen to you talk about your hopes and fears. This may be a friend or family member. The concern and understanding of a counselor, medical social worker, clergy member or support group also may be helpful.
Ask your health care provider about support groups in your area. Or look online, check the phone book, library or a national organization, such as the American Stroke Association or the Aneurysm and AVM Foundation.
Preparing for an appointment
A brain AVM may be diagnosed in an emergency immediately after bleeding has occurred. It may also be detected after other symptoms prompt a brain scan.
But in some cases, a brain AVM may be found during diagnosis or treatment of an unrelated medical condition. You may then be referred to a specialist trained in brain and nervous system conditions (neurologist or neurosurgeon).
Because there's often a lot to discuss, it's a good idea to arrive prepared for your appointment. Here are some tips to help you get ready for your appointment, and what to expect from your care provider.
What you can do
- Be aware of any pre-appointment restrictions. At the time you make the appointment, be sure to ask if there's anything you need to do in advance.
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Make a list of all medications, vitamins and supplements that you're taking.
- Ask a family member or friend to come with you, if possible. Sometimes it can be difficult to absorb all the information provided to you during an appointment. Someone who accompanies you may remember something that you forgot or missed.
- Write down questions to ask. Don't be afraid to ask questions that may come up during your appointment.
Your appointment time is limited, so preparing a list of questions ahead of time will help you make the most of your time together. For brain AVM, some basic questions to ask include:
- What are other possible causes for my symptoms?
- What tests are needed to confirm the diagnosis?
- What are my treatment options and the pros and cons for each?
- What results can I expect?
- What kind of follow-up should I expect?
What to expect from your doctor
Your neurologist is likely to ask about any symptoms you may be experiencing, conduct a physical exam and schedule tests to confirm the diagnosis.
The tests gather information about the size and location of the AVM to help direct your treatment options. Your neurologist may ask:
- When did your symptoms start?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
What you can do in the meantime
Avoid any activity that may raise your blood pressure and put strain on a brain AVM, such as heavy lifting or straining. Also avoid taking any blood-thinning medications, such as warfarin (Jantovin).
Copyright © 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.