Congenital mitral valve anomalies are heart problems present at birth (congenital heart defects) that affect the valve between the heart's upper left chamber (left atrium) and lower left chamber (left ventricle).
Mitral valve anomalies include:
- Thick or stiff valve flaps (leaflets)
- Deformed leaflets or leaflets that join together (fused)
- Problems with the cords that support the valve such as missing cords, short and thick cords, or cords attaching to the heart muscle near the mitral valve
- Heart tissue or heart muscle problems near the mitral valve
- More than one opening in the area of the mitral valve (double-orifice valve)
Types of heart valve disease caused by mitral valve anomalies include:
- Narrowing of the valve (mitral valve stenosis). Stiffening of the leaflets and narrowing of the opening of the mitral valve reduces blood flow from the left atrium to the left ventricle.
- Leaky mitral valve (mitral valve regurgitation). In this condition, the mitral valve flaps don't close tightly or they bulge backward (mitral valve prolapse) into the left atrium as your heart squeezes (contracts). As a result, the mitral valve leaks blood.
You can have both mitral valve stenosis and mitral valve regurgitation.
People with mitral valve anomalies also often have other congenital heart defects.
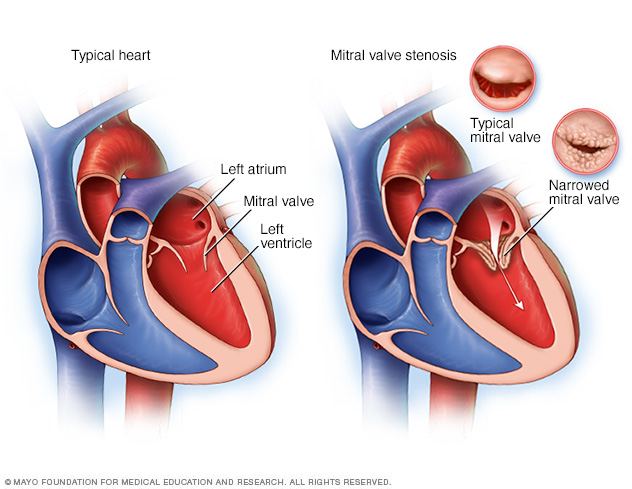
Mitral valve stenosis, shown in the heart on the right, is a condition in which the heart's mitral valve is narrowed. The valve doesn't open properly, blocking blood flow coming into the left ventricle, the main pumping chamber of the heart. A typical heart is shown on the left.
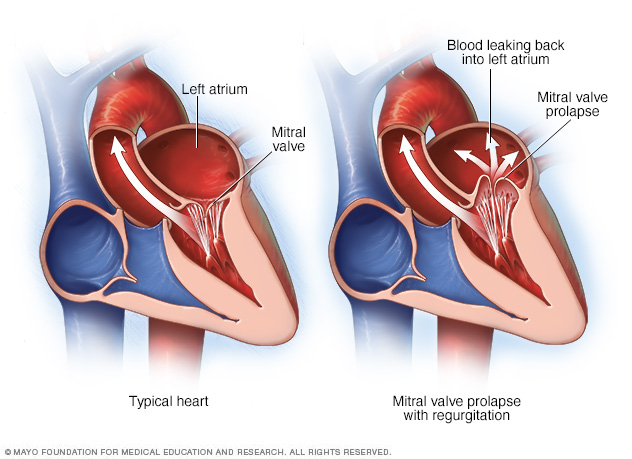
The mitral valve separates the two chambers of the left side of the heart. In mitral valve prolapse, the valve flaps bulge (prolapse) into the upper left chamber (atrium) during each heartbeat. Mitral valve prolapse can cause blood to leak backward, a condition called mitral valve regurgitation.
Diagnosis
Your doctor will do a physical exam and ask questions about your signs and symptoms and your medical and family history. Your doctor will listen to your heart with a stethoscope to check for a heart murmur, which can be a sign of mitral valve disease.
An echocardiogram is the main test used to diagnose congenital mitral valve anomalies. In an echocardiogram, sound waves create video images of your heart in motion. An echocardiogram can show the structure of the heart and heart valves and blood flow through the heart.
There are two types of echocardiograms. During a standard (transthoracic) echocardiogram, the technician presses a device (transducer) firmly against your skin, aiming an ultrasound beam through your chest to your heart. The transducer records the sound wave echoes from your heart. A computer converts the echoes into moving images.
If a standard echocardiogram doesn't give your doctor enough information, you may need a transesophageal echocardiogram. During this test, a flexible probe containing the transducer is guided down your throat and into the tube connecting your mouth to your stomach (esophagus).
Other tests, such as a chest X-ray or electrocardiogram (ECG or EKG), also may be done.
Treatment
Treatment of congenital mitral valve anomalies depends on your signs and symptoms and how severe your condition is. Your doctor may monitor your condition with regular checkups.
You may eventually need surgery to repair or replace the mitral valve.
Mitral valve repair
Your doctor may recommend mitral valve repair when possible, as it saves your heart valve. Surgeons may do one or more of the following during mitral valve repair:
- Patch holes in a valve
- Reconnect valve flaps
- Separate valve flaps that have fused
- Separate, remove or reshape muscle near the valve
- Separate, shorten, lengthen or replace the cords that support the valve
- Remove excess valve tissue so that the leaflets can close tightly
- Tighten or reinforce the ring around a valve (annulus) using an artificial ring
Mitral valve replacement
If the mitral valve can't be repaired, your doctor may recommend mitral valve replacement. In mitral valve replacement, your surgeon removes the damaged valve and replaces it with a mechanical valve or a valve made from cow, pig or human heart tissue (biological tissue valve).
Biological tissue valves wear down over time and eventually need to be replaced. If you have a mechanical valve, you'll need to take blood-thinning medications for life to prevent blood clots. Your doctor will discuss with you the benefits and risks of each type of valve and discuss which valve may be appropriate for you.
Biological tissue valves and mechanical valves may be used in children and adults. The specific valve used is chosen by the cardiologist, surgeon and family after evaluating the risks and benefits.
Follow-up care
Children and adults who have had surgery for congenital mitral valve anomalies or who have congenital mitral valve anomalies will need lifelong care provided by doctors trained in congenital heart conditions, such as pediatric and adult congenital cardiologists. Children and adults will need regular follow-up appointments to monitor for any changes in their condition. Sometime people need repeat valve repair or other surgeries to replace a valve that no longer works.
Copyright © 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.