Endometrial cancer is a type of cancer that begins in the uterus. The uterus is the hollow, pear-shaped pelvic organ where fetal development occurs.
Endometrial cancer begins in the layer of cells that form the lining (endometrium) of the uterus. Endometrial cancer is sometimes called uterine cancer. Other types of cancer can form in the uterus, including uterine sarcoma, but they are much less common than endometrial cancer.
Endometrial cancer is often detected at an early stage because it frequently produces abnormal vaginal bleeding. If endometrial cancer is discovered early, removing the uterus surgically often cures endometrial cancer.
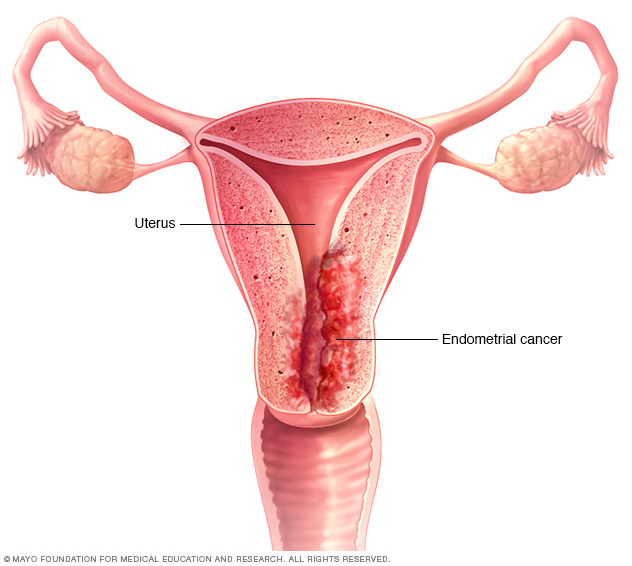
Endometrial cancer begins in the lining (endometrium) of the uterus.
Symptoms
Signs and symptoms of endometrial cancer may include:
- Vaginal bleeding after menopause
- Bleeding between periods
- Pelvic pain
When to see a doctor
Make an appointment with your doctor if you experience any persistent signs or symptoms that worry you.
Causes
Doctors don't know what causes endometrial cancer. What's known is that something occurs to create changes (mutations) in the DNA of cells in the endometrium — the lining of the uterus.
The mutation turns normal, healthy cells into abnormal cells. Healthy cells grow and multiply at a set rate, eventually dying at a set time. Abnormal cells grow and multiply out of control, and they don't die at a set time. The accumulating abnormal cells form a mass (tumor). Cancer cells invade nearby tissues and can separate from an initial tumor to spread elsewhere in the body (metastasize).
Risk factors
Factors that increase the risk of endometrial cancer include:
-
Changes in the balance of female hormones in the body. The ovaries make two main female hormones — estrogen and progesterone. Fluctuations in the balance of these hormones cause changes in the endometrium.
A disease or condition that increases the amount of estrogen, but not the level of progesterone, in your body can increase your risk of endometrial cancer. Examples include irregular ovulation patterns, which might happen in polycystic ovary syndrome, obesity and diabetes. Taking hormones after menopause that contain estrogen but not progesterone increases the risk of endometrial cancer.
A rare type of ovarian tumor that secretes estrogen also can increase the risk of endometrial cancer.
- More years of menstruation. Starting menstruation at an early age — before age 12 — or beginning menopause later increases the risk of endometrial cancer. The more periods you've had, the more exposure your endometrium has had to estrogen.
- Never having been pregnant. If you've never been pregnant, you have a higher risk of endometrial cancer than someone who has had at least one pregnancy.
- Older age. As you get older, your risk of endometrial cancer increases. Endometrial cancer occurs most often after menopause.
- Obesity. Being obese increases your risk of endometrial cancer. This may occur because excess body fat alters your body's balance of hormones.
- Hormone therapy for breast cancer. Taking the hormone therapy drug tamoxifen for breast cancer can increase the risk of developing endometrial cancer. If you're taking tamoxifen, discuss this risk with your doctor. For most, the benefits of tamoxifen outweigh the small risk of endometrial cancer.
- An inherited colon cancer syndrome. Lynch syndrome, also called hereditary nonpolyposis colorectal cancer (HNPCC), is a syndrome that increases the risk of colon cancer and other cancers, including endometrial cancer. Lynch syndrome is caused by a gene mutation passed from parents to children. If a family member has been diagnosed with Lynch syndrome, discuss your risk of the genetic syndrome with your doctor. If you've been diagnosed with Lynch syndrome, ask your doctor what cancer screening tests you should undergo.
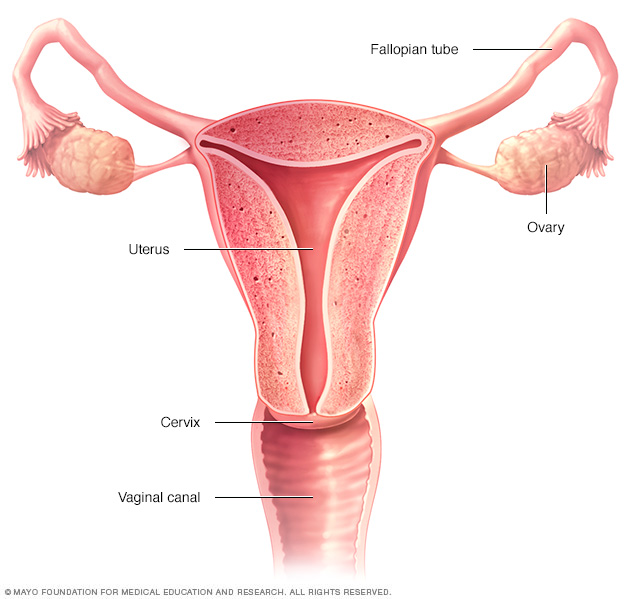
The ovaries, fallopian tubes, uterus, cervix and vagina (vaginal canal) make up the female reproductive system.
Prevention
To reduce your risk of endometrial cancer, you may wish to:
- Talk to your doctor about the risks of hormone therapy after menopause. If you're considering hormone replacement therapy to help control menopause symptoms, talk to your doctor about the risks and benefits. Unless you've undergone a hysterectomy, replacing estrogen alone after menopause may increase your risk of endometrial cancer. Taking a combination of estrogen and progestin can reduce this risk. Hormone therapy carries other risks, so weigh the benefits and risks with your doctor.
- Consider taking birth control pills. Using oral contraceptives for at least one year may reduce endometrial cancer risk. The risk reduction is thought to last for several years after you stop taking oral contraceptives. Oral contraceptives have side effects, though, so discuss the benefits and risks with your doctor.
- Maintain a healthy weight. Obesity increases the risk of endometrial cancer, so work to achieve and maintain a healthy weight. If you need to lose weight, increase your physical activity and reduce the number of calories you eat each day.
Diagnosis
Diagnosing endometrial cancer
Tests and procedures used to diagnose endometrial cancer include:
- Examining the pelvis. During a pelvic exam, your doctor carefully inspects the outer portion of your genitals (vulva), and then inserts two fingers of one hand into your vagina and simultaneously presses the other hand on your abdomen to feel your uterus and ovaries. He or she also inserts a device called a speculum into your vagina. The speculum opens your vagina so that your doctor can view your vagina and cervix for abnormalities.
- Using sound waves to create a picture of your uterus. Your doctor may recommend a transvaginal ultrasound to look at the thickness and texture of the endometrium and help rule out other conditions. In this procedure, a wandlike device (transducer) is inserted into your vagina. The transducer uses sound waves to create a video image of your uterus. This test helps your doctor look for abnormalities in your uterine lining.
- Using a scope to examine your endometrium. During a hysteroscopy, your doctor inserts a thin, flexible, lighted tube (hysteroscope) through your vagina and cervix into your uterus. A lens on the hysteroscope allows your doctor to examine the inside of your uterus and the endometrium.
- Removing a sample of tissue for testing. To get a sample of cells from inside your uterus, you'll likely undergo an endometrial biopsy. This involves removing tissue from your uterine lining for laboratory analysis. Endometrial biopsy may be done in your doctor's office and usually doesn't require anesthesia.
- Performing surgery to remove tissue for testing. If enough tissue can't be obtained during a biopsy or if the biopsy results are unclear, you'll likely need to undergo a procedure called dilation and curettage (D&C). During D&C, tissue is scraped from the lining of your uterus and examined under a microscope for cancer cells.
If endometrial cancer is found, you'll likely be referred to a doctor who specializes in treating cancers involving the female reproductive system (gynecologic oncologist).
Staging endometrial cancer
Once your cancer has been diagnosed, your doctor works to determine the extent (stage) of your cancer. Tests used to determine your cancer's stage may include a chest X-ray, a computerized tomography (CT) scan, positron emission tomography (PET) scan and blood tests. The final determination of your cancer's stage may not be made until after you undergo surgery to treat your cancer.
Your doctor uses information from these tests and procedures to assign your cancer a stage. The stages of endometrial cancer are indicated using Roman numerals ranging from I to IV, with the lowest stage indicating that the cancer hasn't grown beyond the uterus. By stage IV, the cancer has grown to involve nearby organs, such as the bladder, or has spread to distant areas of the body.
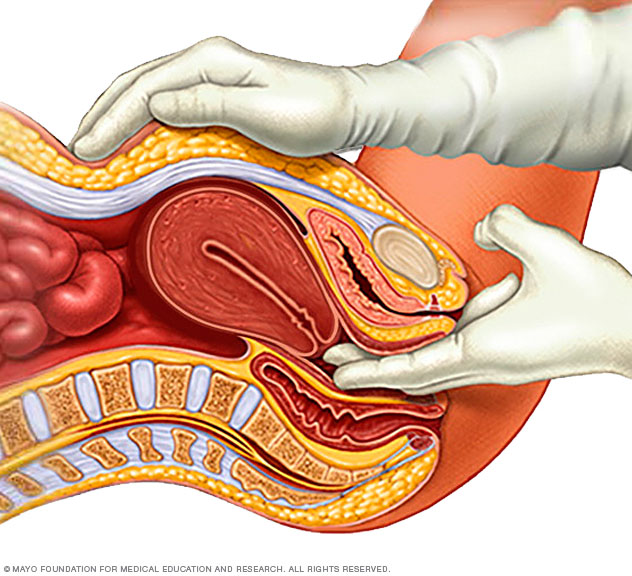
During a pelvic exam, your doctor inserts two gloved fingers inside your vagina. While simultaneously pressing down on your abdomen, he or she can evaluate your uterus, ovaries and other pelvic organs.
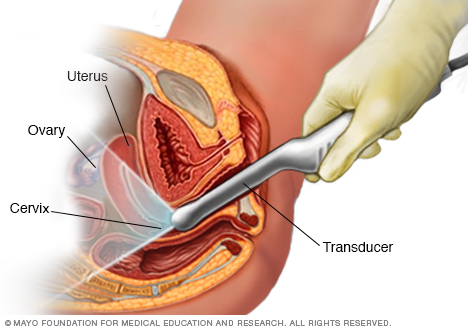
During a transvaginal ultrasound, your care provider or a medical technician inserts a wandlike device (transducer) into your vagina while you lie on your back on an exam table. The transducer emits sound waves that generate images of your pelvic organs.
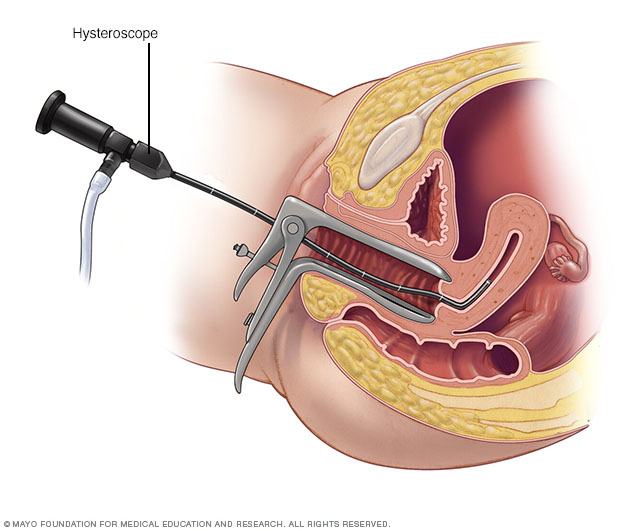
During a hysteroscopy, your provider uses a thin, lighted instrument (hysteroscope) to view the inside of your uterus.
Treatment
Treatment for endometrial cancer is usually with surgery to remove the uterus, fallopian tubes and ovaries. Another option is radiation therapy with powerful energy. Drug treatments for endometrial cancer include chemotherapy with powerful drugs and hormone therapy to block hormones that cancer cells rely on. Other options might be targeted therapy with drugs that attack specific weaknesses in the cancer cells and immunotherapy to help your immune system fight cancer.
Surgery
Treatment for endometrial cancer usually involves an operation to remove the uterus (hysterectomy), as well as to remove the fallopian tubes and ovaries (salpingo-oophorectomy). A hysterectomy makes it impossible for you to become pregnant in the future. Also, once your ovaries are removed, you'll experience menopause, if you haven't already.
During surgery, your surgeon will also inspect the areas around your uterus to look for signs that cancer has spread. Your surgeon may also remove lymph nodes for testing. This helps determine your cancer's stage.
Radiation therapy
Radiation therapy uses powerful energy beams, such as X-rays and protons, to kill cancer cells. In some instances, your doctor may recommend radiation to reduce your risk of a cancer recurrence after surgery. In certain situations, radiation therapy may also be recommended before surgery, to shrink a tumor and make it easier to remove.
If you aren't healthy enough to undergo surgery, you may opt for radiation therapy only.
Radiation therapy can involve:
- Radiation from a machine outside your body. During external beam radiation, you lie on a table while a machine directs radiation to specific points on your body.
- Radiation placed inside your body. Internal radiation (brachytherapy) involves placing a radiation-filled device, such as small seeds, wires or a cylinder, inside your vagina for a short period of time.
Chemotherapy
Chemotherapy uses chemicals to kill cancer cells. You may receive one chemotherapy drug, or two or more drugs can be used in combination. You may receive chemotherapy drugs by pill (orally) or through your veins (intravenously). These drugs enter your bloodstream and then travel through your body, killing cancer cells.
Chemotherapy is sometimes recommended after surgery if there's an increased risk that the cancer might return. It can also be used before surgery to shrink the cancer so that it's more likely to be removed completely during surgery.
Chemotherapy may be recommended for treating advanced or recurrent endometrial cancer that has spread beyond the uterus.
Hormone therapy
Hormone therapy involves taking medications to lower the hormone levels in the body. In response, cancer cells that rely on hormones to help them grow might die. Hormone therapy may be an option if you have advanced endometrial cancer that has spread beyond the uterus.
Targeted drug therapy
Targeted drug treatments focus on specific weaknesses present within cancer cells. By blocking these weaknesses, targeted drug treatments can cause cancer cells to die. Targeted drug therapy is usually combined with chemotherapy for treating advanced endometrial cancer.
Immunotherapy
Immunotherapy is a drug treatment that helps your immune system to fight cancer. Your body's disease-fighting immune system might not attack cancer because the cancer cells produce proteins that blind the immune system cells. Immunotherapy works by interfering with that process. For endometrial cancer, immunotherapy might be considered if the cancer is advanced and other treatments haven't helped.
Supportive (palliative) care
Palliative care is specialized medical care that focuses on providing relief from pain and other symptoms of a serious illness. Palliative care specialists work with you, your family and your other doctors to provide an extra layer of support that complements your ongoing care. Palliative care can be used while undergoing other aggressive treatments, such as surgery, chemotherapy or radiation therapy.
When palliative care is used along with all of the other appropriate treatments, people with cancer may feel better and live longer.
Palliative care is provided by a team of doctors, nurses and other specially trained professionals. Palliative care teams aim to improve the quality of life for people with cancer and their families. This form of care is offered alongside curative or other treatments you may be receiving.
Coping and support
After you receive a diagnosis of endometrial cancer, you may have many questions, fears and concerns. Every person eventually finds a way to cope with an endometrial cancer diagnosis. In time, you'll find what works for you. Until then, you might try to:
- Find out enough about endometrial cancer to make decisions about your care. Find out enough about your cancer so that you feel comfortable about making treatment choices. Ask your doctor about the stage, your treatment options and their side effects. In addition to talking with your doctor, look for information in your local library and on the internet. Good sources of information include the National Cancer Institute and the American Cancer Society.
- Maintain a strong support system. Strong relationships may help you cope with treatment. Talk with close friends and family members about how you're feeling. Connect with other cancer survivors through support groups in your community or online. Ask your doctor about support groups in your area.
- Stay involved in your usual activities when you can. When you're feeling up to it, try to stay involved in your usual activities.
Preparing for an appointment
Make an appointment with your primary care doctor or a gynecologist if you have signs and symptoms that worry you. If you're diagnosed with endometrial cancer, you're likely to be referred to a doctor who specializes in cancers of the female reproductive system (gynecologic oncologist).
Because appointments can be brief and there's often a lot to discuss, it's a good idea to be well prepared. Here's some information to help you get ready, and what you can expect from your doctor.
What you can do
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Make a list of all medications, vitamins and supplements that you're taking. Also note if you've used any type of hormonal therapy in the past, including birth control pills, tamoxifen or other hormonal treatments.
- Ask a family member or friend to accompany you. Sometimes it can be difficult to absorb all the information provided during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Write down questions to ask your doctor.
Your time with your doctor is limited, so preparing a list of questions ahead of time can help you make the most of your time together. List your questions from most important to least important in case time runs out. For endometrial cancer, some basic questions to ask your doctor include:
- What's the most likely cause of my symptoms?
- Are there any other possible causes for my symptoms?
- What tests do I need to diagnose endometrial cancer?
- Are there other tests for staging the cancer?
- What treatments are available? What side effects can I expect from each treatment? How will these treatments affect my sexuality?
- What do you feel is the best course of action for me?
- What are the alternatives to the primary approach that you're suggesting?
- I have other health conditions. How can I best manage them together?
- Are there any restrictions that I need to follow?
- Has my cancer spread? What stage is it?
- What's my prognosis?
- Should I see a specialist? What will that cost, and will my insurance cover it?
- Are there any brochures or other printed material that I can take with me? What websites do you recommend?
In addition to the questions that you've prepared to ask your doctor, don't hesitate to ask additional questions during your appointment.
What to expect from your doctor
Your doctor will likely have questions for you. If you're ready to answer them, it may help reserve time to go over points you want to spend more time on. Your doctor may ask:
- Have you experienced any unusual vaginal bleeding or discharge? How often does that occur?
- Do you have any pelvic pain?
- Have you had any other symptoms?
- Have your symptoms been continuous or occasional?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
- Have you taken estrogen-only hormone therapy for menopausal symptoms?
- Do you have any personal history of cancer?
- Have other members of your family been diagnosed with cancer? How old was each relative when he or she was diagnosed? What types of cancer?
Copyright © 1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.