Graves' disease is an immune system disorder that results in the overproduction of thyroid hormones (hyperthyroidism). Although a number of disorders may result in hyperthyroidism, Graves' disease is a common cause.
Thyroid hormones affect many body systems, so signs and symptoms of Graves' disease can be wide ranging. Although Graves' disease may affect anyone, it's more common among women and in people younger than age 40.
The primary treatment goals are to reduce the amount of thyroid hormones that the body produces and lessen the severity of symptoms.

Your thyroid gland is located at the base of your neck, just below the Adam's apple.
Symptoms
Common signs and symptoms of Graves' disease include:
- Anxiety and irritability
- A fine tremor of the hands or fingers
- Heat sensitivity and an increase in perspiration or warm, moist skin
- Weight loss, despite normal eating habits
- Enlargement of the thyroid gland (goiter)
- Change in menstrual cycles
- Erectile dysfunction or reduced libido
- Frequent bowel movements
- Bulging eyes (Graves' ophthalmopathy)
- Fatigue
- Thick, red skin usually on the shins or tops of the feet (Graves' dermopathy)
- Rapid or irregular heartbeat (palpitations)
- Sleep disturbance
Graves' ophthalmopathy
About 30% of people with Graves' disease show some signs and symptoms of Graves' ophthalmopathy. In Graves' ophthalmopathy, inflammation and other immune system events affect muscles and other tissues around your eyes. Signs and symptoms may include:
- Bulging eyes
- Gritty sensation in the eyes
- Pressure or pain in the eyes
- Puffy or retracted eyelids
- Reddened or inflamed eyes
- Light sensitivity
- Double vision
- Vision loss
Graves' dermopathy
An uncommon manifestation of Graves' disease, called Graves' dermopathy, is the reddening and thickening of the skin, most often on your shins or the tops of your feet.
When to see a doctor
A number of medical conditions can cause the signs and symptoms associated with Graves' disease. See your doctor if you experience any potential problems related to Graves' disease to get a prompt and accurate diagnosis.
Seek emergency care if you're experiencing heart-related signs and symptoms, such as a rapid or irregular heartbeat, or if you develop vision loss.
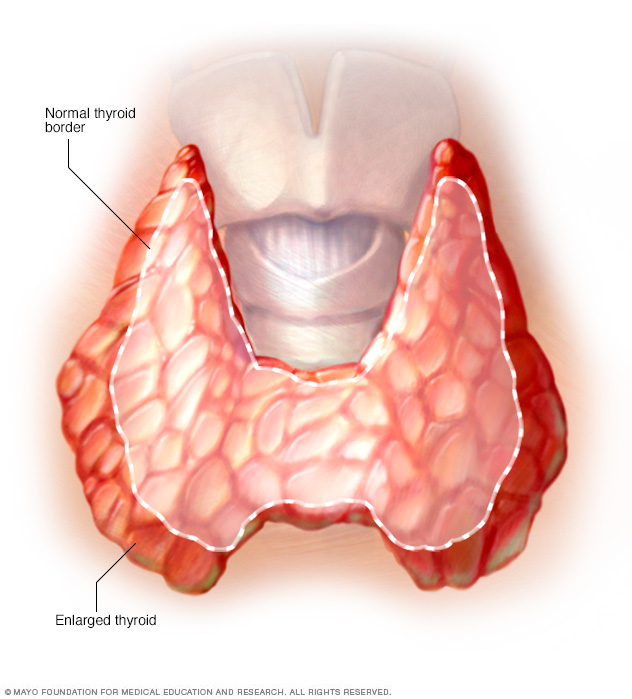
Widespread enlargement of the thyroid can expand the gland well beyond its typical size (left) and cause a noticeable bulge in the neck (right).
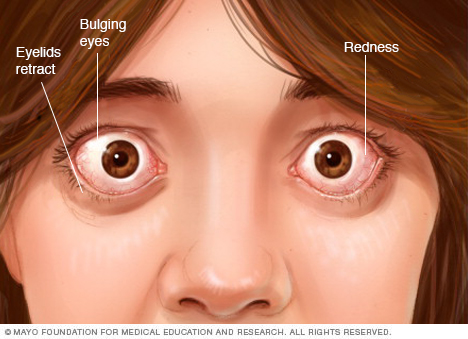
Graves' ophthalmopathy signs and symptoms include bulging eyes, redness and retracting eyelids.

Rarely, people who have Graves' disease develop a reddish thickening of the skin that resembles the texture of an orange peel (Graves' dermopathy). This results from a buildup of protein in the skin. It often occurs on the shins and on the tops of the feet.
Causes
Graves' disease is caused by a malfunction in the body's disease-fighting immune system. It's unknown why this happens.
The immune system normally produces antibodies designed to target a specific virus, bacterium or other foreign substance. In Graves' disease — for reasons that aren't well understood — the immune system produces an antibody to one part of the cells in the hormone-producing gland in the neck (thyroid gland).
Normally, thyroid function is regulated by a hormone released by a tiny gland at the base of the brain (pituitary gland). The antibody associated with Graves' disease — thyrotropin receptor antibody (TRAb) — acts like the regulatory pituitary hormone. That means that TRAb overrides the normal regulation of the thyroid, causing an overproduction of thyroid hormones (hyperthyroidism).
Cause of Graves' ophthalmopathy
Graves' ophthalmopathy results from a buildup of certain carbohydrates in the muscles and tissues behind the eyes — the cause of which also isn't known. It appears that the same antibody that can cause thyroid dysfunction may also have an "attraction" to tissues surrounding the eyes.
Graves' ophthalmopathy often appears at the same time as hyperthyroidism or several months later. But signs and symptoms of ophthalmopathy may appear years before or after the onset of hyperthyroidism. Graves' ophthalmopathy can also occur even if there's no hyperthyroidism.
Risk factors
Although anyone can develop Graves' disease, many factors can increase the risk of disease, including:
- Family history. Because a family history of Graves' disease is a known risk factor, there is likely a gene or genes that can make a person more susceptible to the disorder.
- Sex. Women are much more likely to develop Graves' disease than are men.
- Age. Graves' disease usually develops in people before age 40.
- Other autoimmune disorders. People with other disorders of the immune system, such as type 1 diabetes or rheumatoid arthritis, have an increased risk.
- Emotional or physical stress. Stressful life events or illness may act as a trigger for the onset of Graves' disease among people who have genes that increase their risk.
- Pregnancy. Pregnancy or recent childbirth may increase the risk of the disorder, particularly among women who have genes that increase their risk.
- Smoking. Cigarette smoking, which can affect the immune system, increases the risk of Graves' disease. Smokers who have Graves' disease are also at increased risk of developing Graves' ophthalmopathy.
Complications
Complications of Graves' disease can include:
- Pregnancy issues. Possible complications of Graves' disease during pregnancy include miscarriage, preterm birth, fetal thyroid dysfunction, poor fetal growth, maternal heart failure and preeclampsia. Preeclampsia is a maternal condition that results in high blood pressure and other serious signs and symptoms.
- Heart disorders. If left untreated, Graves' disease can lead to heart rhythm disorders, changes in the structure and function of the heart muscles, and the inability of the heart to pump enough blood to the body (heart failure).
-
Thyroid storm. A rare but life-threatening complication of Graves' disease is thyroid storm, also known as accelerated hyperthyroidism or thyrotoxic crisis. It's more likely when severe hyperthyroidism is untreated or treated inadequately.
The sudden and drastic increase in thyroid hormones can produce many effects, including fever, sweating, vomiting, diarrhea, delirium, severe weakness, seizures, irregular heartbeat, yellow skin and eyes (jaundice), severe low blood pressure, and coma. Thyroid storm requires immediate emergency care.
- Brittle bones. Untreated hyperthyroidism also can lead to weak, brittle bones (osteoporosis). The strength of your bones depends, in part, on the amount of calcium and other minerals they contain. Too much thyroid hormone interferes with your body's ability to incorporate calcium into your bones.
Diagnosis
To diagnose Graves' disease, your doctor may conduct a physical exam and check for signs and symptoms of Graves' disease. He or she may also discuss your medical and family history. Your doctor may also order tests including:
-
Blood tests. Blood tests can help your doctor determine your levels of thyroid-stimulating hormone (TSH) — the pituitary hormone that normally stimulates the thyroid gland — and your levels of thyroid hormones. People with Graves' disease usually have lower than normal levels of TSH and higher levels of thyroid hormones.
Your doctor may order another lab test to measure the levels of the antibody known to cause Graves' disease. It's usually not needed to diagnose the disease, but results that don't show antibodies might suggest another cause of hyperthyroidism.
- Radioactive iodine uptake. Your body needs iodine to make thyroid hormones. By giving you a small amount of radioactive iodine and later measuring the amount of it in your thyroid gland with a specialized scanning camera, your doctor can determine the rate at which your thyroid gland takes up iodine. The amount of radioactive iodine taken up by the thyroid gland helps determine if Graves' disease or another condition is the cause of the hyperthyroidism. This test may be combined with a radioactive iodine scan to show a visual image of the uptake pattern.
- Ultrasound. Ultrasound uses high-frequency sound waves to produce images of structures inside the body. It can show if the thyroid gland is enlarged. It's most useful in people who can't undergo radioactive iodine uptake, such as pregnant women.
- Imaging tests. If the diagnosis of Graves' disease isn't clear from a clinical assessment, your doctor may order special imaging tests, such as a CT scan or MRI.
Treatment
The treatment goals for Graves' disease are to stop the production of thyroid hormones and to block the effect of the hormones on the body. Some treatments include:
Radioactive iodine therapy
With this therapy, you take radioactive iodine (radioiodine) by mouth. Because the thyroid needs iodine to produce hormones, the thyroid takes the radioiodine into the thyroid cells and the radiation destroys the overactive thyroid cells over time. This causes your thyroid gland to shrink, and symptoms lessen gradually, usually over several weeks to several months.
Radioiodine therapy may increase your risk of new or worsened symptoms of Graves' ophthalmopathy. This side effect is usually mild and temporary, but the therapy may not be recommended if you already have moderate to severe eye problems.
Other side effects may include tenderness in the neck and a temporary increase in thyroid hormones. Radioiodine therapy isn't used for treating pregnant women or women who are breast-feeding.
Because this treatment causes thyroid activity to decline, you'll likely need treatment later to supply your body with normal amounts of thyroid hormones.
Anti-thyroid medications
Anti-thyroid medications interfere with the thyroid's use of iodine to produce hormones. These prescription medications include propylthiouracil and methimazole (Tapazole).
Because the risk of liver disease is more common with propylthiouracil, methimazole is considered the first choice when doctors prescribe medication. However, propylthiouracil is the preferred anti-thyroid drug during the first trimester of pregnancy, as methimazole has a slight risk of birth defects. Pregnant women will generally go back to taking methimazole after the first trimester.
When these two drugs are used alone without other treatments, a relapse of hyperthyroidism may occur at a later time. Taking either drug for longer than a year may result in better long-term results. Anti-thyroid drugs may also be used before or after radioiodine therapy as a supplemental treatment.
Side effects of both drugs include rash, joint pain, liver failure or a decrease in disease-fighting white blood cells.
Beta blockers
These medications don't inhibit the production of thyroid hormones, but they do block the effect of hormones on the body. They may provide fairly rapid relief of irregular heartbeats, tremors, anxiety or irritability, heat intolerance, sweating, diarrhea, and muscle weakness.
Beta blockers include:
- Propranolol (Inderal, InnoPran XL)
- Atenolol (Tenormin)
- Metoprolol (Lopressor, Toprol-XL)
- Nadolol (Corgard)
Beta blockers aren't often prescribed for people with asthma because the drugs may trigger an asthma attack. These drugs may also complicate management of diabetes.
Surgery
Surgery to remove all or part of your thyroid (thyroidectomy or subtotal thyroidectomy) also is an option for the treatment of Graves' disease. After the surgery, you'll likely need treatment to supply your body with normal amounts of thyroid hormones.
Risks of this surgery include potential damage to the nerve that controls your vocal cords and the tiny glands located adjacent to your thyroid gland (parathyroid glands). Your parathyroid glands produce a hormone that controls the level of calcium in your blood. Complications are rare under the care of a surgeon experienced in thyroid surgery. You'll need to take thyroid medication for life after this surgery.
Treating Graves' ophthalmopathy
Mild symptoms of Graves' ophthalmopathy may be managed by using over-the-counter artificial tears during the day and lubricating gels at night. If your symptoms are more severe, your doctor may recommend:
- Corticosteroids. Treatment with corticosteroids, such as prednisone, may lessen swelling behind your eyeballs. Side effects may include fluid retention, weight gain, elevated blood sugar levels, increased blood pressure and mood swings.
- Teprotumumab (Tepezza). This medication may be used to treat Graves' ophthalmopathy. It's given through an IV in the arm every three weeks and is given eight times. It can cause side effects such as nausea, diarrhea, muscle spasms and elevated blood sugar levels. As this medication is new, its role in the management of Graves' opthalmopathy isn't yet defined.
- Prisms. You may have double vision either because of Graves' disease or as a side effect of surgery for Graves' disease. Though they don't work for everyone, prisms in your glasses may correct your double vision.
-
Orbital decompression surgery. In this surgery, your doctor removes the bone between your eye socket (orbit) and your sinuses — the air spaces next to the orbit. This gives your eyes room to move back to their original position.
This treatment is usually used if pressure on the optic nerve threatens the loss of vision. Possible complications include double vision.
- Orbital radiotherapy. This was once a common treatment for this condition, but the benefits aren't clear. It uses targeted X-rays over the course of several days to destroy some of the tissue behind your eyes. Your doctor may recommend this if your eye problems are worsening and corticosteroids alone aren't effective or well tolerated.
Graves' ophthalmopathy doesn't always improve with treatment of Graves' disease. Symptoms of Graves' ophthalmopathy may even get worse for three to six months. After that, the signs and symptoms of Graves' ophthalmopathy usually become stable for a year or so and then begin to get better, often on their own.
Lifestyle and home remedies
If you have Graves' disease, make your mental and physical well-being a priority:
- Eating well and exercising can enhance the improvement in some symptoms during treatment and help you feel better in general. For example, because your thyroid controls your metabolism, you may have a tendency to gain weight when the hyperthyroidism is corrected. Brittle bones also can occur with Graves' disease, and weight-bearing exercises can help maintain bone density.
- Easing stress may be helpful, as stress may trigger or worsen Graves' disease. Listening to music, taking a warm bath or walking can help relax you and put you in a better frame of mind. Partner with your doctor to develop a plan that involves including good nutrition, exercise and relaxation into your daily routine.
For Graves' ophthalmopathy
These steps may make your eyes feel better if you have Graves' ophthalmopathy:
- Apply cool compresses to your eyes. The added moisture may soothe your eyes.
- Wear sunglasses. When your eyes protrude, they're more vulnerable to ultraviolet rays and more sensitive to bright light. Wearing sunglasses that wrap around the sides of your head will also lessen the irritation of your eyes from the wind.
- Use lubricating eyedrops. Eyedrops may relieve the dry, scratchy sensation on the surface of your eyes. A paraffin-based gel can be applied at night.
- Elevate the head of your bed. Keeping your head higher than the rest of your body lessens fluid accumulation in the head and may relieve the pressure on your eyes.
- Don't smoke. Smoking worsens Graves' ophthalmopathy.
For Graves' dermopathy
If the disease affects your skin (Graves' dermopathy), use over-the-counter creams or ointments containing hydrocortisone to relieve swelling and reddening. In addition, using compression wraps on your legs may help.
Preparing for an appointment
You'll probably see your primary care doctor first. You may be referred to a specialist in disorders of hormone function and the endocrine system (endocrinologist). If you have Graves' ophthalmopathy, your doctor may also recommend that you see a doctor who has trained in eye disorders (ophthalmologist).
Here's some information to help you get ready for your appointment, and what to expect from your doctor.
What you can do
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Write down key personal information, including your family medical history, and any major stresses or recent life changes.
- Make a list of all medications, vitamins or supplements that you're taking. Make note of the dosage of each.
- Write down questions to ask your doctor.
Preparing a list of questions can help you make the most of your time with your doctor. For Graves' disease, some basic questions to ask your doctor include:
- What's the most likely cause of my symptoms?
- What kinds of tests do I need? Do these tests require any special preparation?
- Is this condition temporary or long lasting?
- What treatments are available, and which do you recommend?
- What types of side effects can I expect from treatment?
- I have other health conditions. How can I best manage these conditions together?
- Where can I find more information on Graves' disease?
What to expect from your doctor
Your doctor is likely to ask you a number of questions. Be prepared to answer the following:
- When did you first notice your symptoms?
- Do you have symptoms all the time or do they come and go?
- Have you recently started a new medication?
- Have you experienced rapid or unintended weight loss? How much have you lost?
- Have you observed any change in your menstrual cycle?
- Have you experienced any sexual dysfunction?
- Are you having trouble sleeping?
Copyright © 1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.