Keratosis pilaris (ker-uh-TOE-sis pih-LAIR-is) is a common, harmless skin condition that causes dry, rough patches and tiny bumps, often on the upper arms, thighs, cheeks or buttocks. The bumps usually don't hurt or itch.
Keratosis pilaris is often considered a variant of normal skin. It can't be cured or prevented. But you can treat it with moisturizers and prescription creams to help improve the appearance of the skin. The condition usually disappears by age 30.

Keratosis pilaris causes small bumps to appear on the upper arms, legs or buttocks. They usually don't hurt or itch.
Symptoms
Keratosis pilaris can occur at any age, but it's more common in young children. Signs and symptoms include:
- Painless tiny bumps, typically on the upper arms, thighs, cheeks or buttocks
- Dry, rough skin in the areas with bumps
- Worsening when seasonal changes cause low humidity and dry skin
- Sandpaper-like bumps resembling goose flesh
When to see a doctor
Treatment for keratosis pilaris usually isn't necessary. But if you're concerned about your or your child's skin, consult your family doctor or a specialist in skin conditions (dermatologist).
Causes
Keratosis pilaris is caused by the buildup of keratin — a hard protein that protects skin from harmful substances and infection. The keratin blocks the opening of hair follicles, causing patches of rough, bumpy skin.
It's not clear why keratin builds up in people with keratosis pilaris. It may occur in association with a genetic disease or with skin conditions such as atopic dermatitis. Dry skin tends to make keratosis pilaris worse.
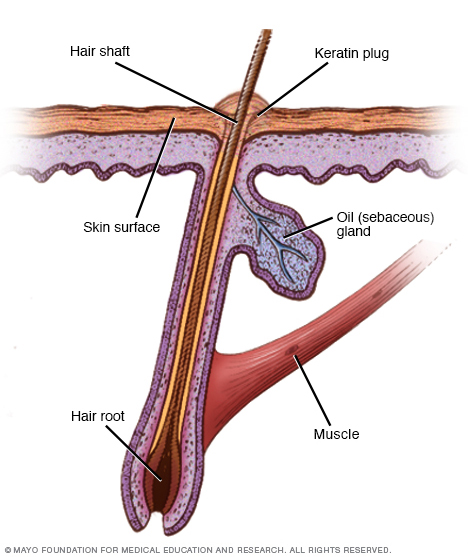
Keratosis pilaris develops when keratin forms a scaly plug that blocks the opening of the hair follicle. Usually plugs form in many hair follicles, causing patches of rough, bumpy skin.
Diagnosis
Your doctor will likely be able to diagnose keratosis pilaris just by looking at the affected skin. No testing is needed.
Treatment
Keratosis pilaris usually clears up on its own gradually. In the meantime, you might use any of the various products available to help improve the appearance of the skin. If moisturizing and other self-care measures don't help, your doctor may prescribe medicated creams.
- Creams to remove dead skin cells. Creams containing alpha hydroxy acid, lactic acid, salicylic acid or urea help loosen and remove dead skin cells. They also moisturize and soften dry skin. Depending on their strengths, these creams (topical exfoliants) are available over-the-counter or with a prescription. Your doctor can advise you on the best option and how often to apply. The acids in these creams may cause redness, stinging or skin irritation, so they aren't recommended for young children.
- Creams to prevent plugged follicles. Creams derived from vitamin A (topical retinoids) work by promoting cell turnover and preventing plugged hair follicles. Tretinoin (Altreno, Avita, Renova, Retin-A, others) and tazarotene (Arazlo, Avage, Tazorac, others) are examples of topical retinoids. These products can irritate and dry the skin. Also, if you're pregnant or nursing, your doctor may suggest delaying topical retinoid therapy or choosing another treatment.
Using medicated cream regularly may improve the appearance of the skin. But if you stop, the condition returns. And even with treatment, keratosis pilaris might last for years.
Lifestyle and home remedies
Self-help measures won't prevent keratosis pilaris or make it go away. But they may improve the appearance of the affected skin. When using a product new to you, test it on one area of affected skin first, such as an arm, to see whether the product works for you and doesn't cause a reaction.
- Use warm water and limit bath time. Hot water and long showers or baths remove oils from the skin. Limit bath or shower time to about 10 minutes or less. Use warm, not hot, water.
- Be gentle to the skin. Avoid harsh, drying soaps. Gently remove dead skin (exfoliate) with a washcloth or loofah. Vigorous scrubbing or removal of hair follicle plugs may irritate the skin and aggravate the condition. After washing or bathing, gently pat or blot the skin with a towel so that some moisture remains.
- Try medicated creams. Apply an over-the-counter cream that contains urea, lactic acid, alpha hydroxy acid or salicylic acid. These creams help loosen and remove dead skin cells. They also moisturize and soften dry skin. Put on this product before moisturizer.
- Moisturize. While the skin is still moist from bathing, apply a moisturizer that contains lanolin, petroleum jelly or glycerin. These ingredients soothe dry skin and help trap moisture. Thicker moisturizers work best, such as Eucerin and Cetaphil. Reapply the product to the affected skin several times a day.
- Use a humidifier. Low humidity dries out the skin. A portable home humidifier or one attached to your furnace will add moisture to the air inside your home.
- Avoid friction from tight clothes. Protect affected skin from the friction caused by wearing tight clothes.
Preparing for an appointment
You're likely to start by seeing your family doctor. Or he or she may refer you to a specialist in skin diseases (dermatologist). You may want to prepare a list of questions to ask your doctor.
For keratosis pilaris, some basic questions include:
- What is likely causing the symptoms?
- What are other possible causes for the symptoms?
- Is this condition likely temporary or chronic?
- What is the best course of action?
- What are the alternatives to the primary approach that you're suggesting?
- Is there a generic alternative to the medicine you're prescribing?
What to expect from your doctor
Your doctor is likely to ask you several questions. Being ready to answer them may reserve time to go over any points you want to discuss more. Your doctor may ask:
- When did the symptoms begin?
- Have the symptoms been continuous or occasional?
- What, if anything, seems to improve the symptoms?
- What, if anything, appears to worsen the symptoms?
- Do other family members have similar skin changes?
- Do you or your child have a history of asthma or hay fever or other allergies?
- Do you or your child have a history of eczema?
Copyright © 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.