Peyronie's (pay-roe-NEEZ) disease is a noncancerous condition resulting from fibrous scar tissue that develops on the penis and causes curved, painful erections. Penises vary in shape and size, and having a curved erection isn't necessarily a cause for concern. But Peyronie's disease causes a significant bend or pain in some men.
This can prevent you from having sex or might make it difficult to get or maintain an erection (erectile dysfunction). For many men, Peyronie's disease also causes stress and anxiety. Penile shortening is another common concern.
Peyronie's disease rarely goes away on its own. In most men with Peyronie's disease, the condition will remain as is or worsen. Early treatment soon after developing the condition may keep it from getting worse or even improve symptoms. Even if you've had the condition for some time, treatment may help improve bothersome symptoms, such as pain, curvature and penile shortening.
Symptoms
Peyronie's disease signs and symptoms might appear suddenly or develop gradually. The most common signs and symptoms include:
- Scar tissue. The scar tissue associated with Peyronie's disease — called plaque but different from plaque that can build up in blood vessels — can be felt under the skin of the penis as flat lumps or a band of hard tissue.
- A significant bend to the penis. Your penis might curve upward or downward or bend to one side.
- Erection problems. Peyronie's disease might cause problems getting or maintaining an erection (erectile dysfunction). But, often men report erectile dysfunction before the beginning of Peyronie's disease symptoms.
- Shortening of the penis. Your penis might become shorter as a result of Peyronie's disease.
- Pain. You might have penile pain, with or without an erection.
- Other penile deformity. In some men with Peyronie's disease, the erect penis might have narrowing, indentations or even an hourglass-like appearance, with a tight, narrow band around the shaft.
The curvature and penile shortening associated with Peyronie's disease might gradually worsen. At some point, however, the condition typically stabilizes after three to 12 months or so.
Pain during erections usually improves within one to two years, but the scar tissue, penile shortening and curvature often remain. In some men, both the curvature and pain associated with Peyronie's disease improve without treatment.
When to see a doctor
See your doctor as soon as possible after you notice signs or symptoms of Peyronie's disease. Early treatment gives you the best chance to improve the condition — or prevent it from getting worse. If you've had the condition for some time, you may wish to see a doctor if the pain, curvature, length or other deformities bother you or your partner.
Causes
The cause of Peyronie's disease isn't completely understood, but a number of factors appear to be involved.
It's thought Peyronie's disease generally results from repeated injury to the penis. For example, the penis might be damaged during sex, athletic activity or as the result of an accident. However, most often, no specific trauma to the penis is recalled.
During the healing process after injury to the penis, scar tissue forms in a disorganized manner. This can lead to a nodule you can feel or development of curvature.
Each side of the penis contains a spongelike tube (corpus cavernosum) that contains many tiny blood vessels. Each of the corpora cavernosa is encased in a sheath of elastic tissue called the tunica albuginea (TOO-nih-kuh al-BYOO-JIN-e-uh), which stretches during an erection.
When you become sexually aroused, blood flow to these chambers increases. As the chambers fill with blood, the penis expands, straightens and stiffens into an erection.
In Peyronie's disease, when the penis becomes erect, the region with the scar tissue doesn't stretch, and the penis bends or becomes disfigured and possibly painful.
In some men, Peyronie's disease comes on gradually and doesn't seem to be related to an injury. Researchers are investigating whether Peyronie's disease might be linked to an inherited trait or certain health conditions.
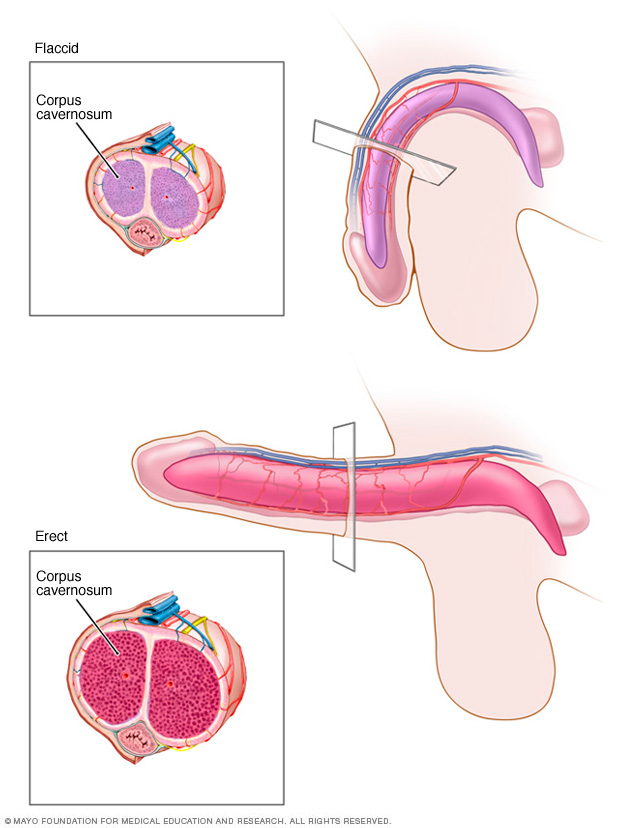
The penis contains two cylindrical, spongelike structures (corpora cavernosa). During sexual arousal, nerve impulses increase blood flow to both of these cylinders. This sudden influx of blood causes an erection by expanding, straightening and stiffening the penis.
Risk factors
Minor injury to the penis doesn't always lead to Peyronie's disease. However, various factors can contribute to poor wound healing and scar tissue buildup that might play a role in Peyronie's disease. These include:
- Heredity. If a family member has Peyronie's disease, you have an increased risk of the condition.
- Connective tissue disorders. Men who have certain connective tissue disorders appear to have an increased risk of developing Peyronie's disease. For example, a number of men who have Peyronie's disease also have a cordlike thickening across the palm that causes the fingers to pull inward (Dupuytren's contracture).
- Age. Peyronie's disease can occur in men of any age, but the prevalence of the condition increases with age, especially for men in their 50s and 60s. Curvature in younger men is less often due to Peyronie's disease and is more commonly called congenital penile curvature. A small amount of curvature in younger men is normal and not concerning.
Other factors — including certain health conditions, smoking and some types of prostate surgery — might be linked to Peyronie's disease.
Complications
Complications of Peyronie's disease might include:
- Inability to have sexual intercourse
- Difficulty achieving or maintaining an erection (erectile dysfunction)
- Anxiety or stress about sexual abilities or the appearance of your penis
- Stress on your relationship with your sexual partner
- Difficulty fathering a child, because intercourse is difficult or impossible
- Reduced penis length
- Penile pain
Diagnosis
A physical exam is often sufficient to identify the presence of scar tissue in the penis and diagnose Peyronie's disease. Rarely, other conditions cause similar symptoms and need to be ruled out.
Tests to diagnose Peyronie's disease and understand exactly what's causing your symptoms might include the following:
-
Physical exam. Your doctor will feel (palpate) your penis when it's not erect, to identify the location and amount of scar tissue. He or she might also measure the length of your penis. If the condition continues to worsen, this initial measurement helps determine whether the penis has shortened.
Your doctor might also ask you to bring in photos of your erect penis taken at home. This can determine the degree of curvature, location of scar tissue or other details that might help identify the best treatment approach.
-
Other tests. Your doctor might order an ultrasound or other tests to examine your penis when it's erect. Before testing, you'll likely receive an injection directly into the penis that causes it to become erect.
Ultrasound is the most commonly used test for penis abnormalities. Ultrasound tests use sound waves to produce images of soft tissues. These tests can show the presence of scar tissue, blood flow to the penis and any other abnormalities.
Treatment
Treatment recommendations for Peyronie's disease depend on how long it's been since you began having symptoms.
- Acute phase. You have penile pain or changes in curvature or length or a deformity of the penis. The acute phase happens early in the disease and may last only two to four weeks but sometimes lasts for up to a year or longer.
- Chronic phase. Your symptoms are stable, and you have no penile pain or changes in curvature, length or deformity of the penis. The chronic phase happens later in the disease and generally occurs around three to 12 months after symptoms begin.
For the acute phase of the disease, treatments range from:
- Recommended. When used early in the disease process, penile traction therapy prevents length loss and minimizes the extent of curvature that occurs.
- Optional. Medical and injection therapies are optional in this phase, with some more effective than others.
- Not recommended. Surgery isn't recommended until the disease stabilizes, to avoid the need for repeat surgery.
For the chronic phase of the disease, several potential treatments are available. They may be done alone or in combination:
- Watchful waiting
- Injection treatments
- Traction therapy
- Surgery
Oral medications aren't recommended in the chronic phase, as they haven't been shown to be effective at this stage of the disease. Shock wave therapy, stem cells and platelet-rich plasma also haven't been shown to be effective in human studies.
Medications
A number of oral medications have been tried to treat Peyronie's disease, but they have not been shown to be effective consistently and are not as effective as surgery.
In some men, drugs injected directly into the penis might reduce curvature and pain associated with Peyronie's disease. Depending on the therapy, you might be given a local anesthetic to prevent pain during the injections.
If you have one of these treatments, you'll likely receive multiple injections over several months. Injection medications may also be used in combination with oral drugs or traction therapies.
Medications include:
-
Collagenase. The only FDA-approved medication for Peyronie's disease is collagenase clostridium histolyticum (Xiaflex). This medicine has been approved for use in adult men with moderate to severe curvatures and a palpable nodule.
This therapy has been shown to improve curvature and bothersome symptoms associated with Peyronie's disease. The treatment works by breaking down the buildup of collagen that causes penile curvature. Collagenase appears to be more effective when used in conjunction with "modeling," which is forcible bending of the penis in the opposite direction of the bend.
- Verapamil. This is a drug normally used to treat high blood pressure. It appears to disrupt the production of collagen, a protein that might be a key factor in the formation of Peyronie's disease scar tissue. The drug is well tolerated and may reduce pain, too.
- Interferon. This is a type of protein that appears to disrupt the production of fibrous tissue and help break it down. One placebo-controlled trial showed improvement using this therapy over placebo. Interferon also has been shown to reduce penile pain in men with Peyronie's disease.
Traction therapy
Penile traction therapy involves stretching the penis with a self-applied mechanical device for a period of time to improve penile length, curvature and deformity.
Depending on the specific device, traction therapy may need to be worn for as little as 30 minutes to as much as three to eight hours a day to achieve benefits. The effectiveness of treatment may also depend on the specific device used.
Traction therapy is recommended in the early phase of Peyronie's disease. It's the only treatment shown to improve penile length. Traction therapy may also be used in the chronic phase of the disease, combined with other treatments or after surgery for a better outcome.
Surgery
Your doctor might suggest surgery if the deformity of your penis is severe, sufficiently bothersome or prevents you from having sex. Surgery usually isn't recommended until you've had the condition for nine to 12 months and the curvature of your penis stops increasing and stabilizes for at least three to six months.
Common surgical methods include:
-
Suturing (plicating) the unaffected side. A variety of procedures can be used to suture (plicate) the longer side of the penis — the side without scar tissue. This results in a straightening of the penis, although this is often limited to less severe curvatures.
Several plication techniques may be used, generally resulting in similar success rates depending on surgeon experience and preference.
-
Incision or excision and grafting. With this type of surgery, the surgeon makes one or more cuts in the scar tissue, allowing the sheath to stretch out and the penis to straighten. The surgeon might remove some of the scar tissue.
A piece of tissue (graft) is often sewn into place to cover the holes in the tunica albuginea. The graft might be tissue from your own body, human or animal tissue, or a synthetic material.
This procedure is generally used in men with more-severe curvature or deformity, such as indentations. This procedure is associated with greater risks of worsening erectile function when compared with the plication procedures.
-
Penile implants. Surgically placed penile implants are inserted into the spongy tissue that fills with blood during an erection. The implants might be semirigid — manually bent down most of the time and bent upward for sexual intercourse.
Another type of implant is inflated with a pump implanted in the scrotum. Penile implants might be considered if you have both Peyronie's disease and erectile dysfunction.
When the implants are put in place, the surgeon might perform additional procedures to improve the curvature if needed.
The type of surgery used will depend on your condition. Your doctor will consider the location of scar tissue, the severity of your symptoms and other factors. If you're uncircumcised, your doctor might recommend a circumcision during surgery.
Depending on the type of surgery you have, you might be able to go home from the hospital the same day or you might need to stay overnight. Your surgeon will advise you on how long you should wait before going back to work — generally, a few days. After surgery for Peyronie's disease, you'll need to wait four to eight weeks before sexual activity.
Other treatments
A technique known as iontophoresis uses an electric current to administer a combination of verapamil and a steroid noninvasively through the skin. Available research has shown conflicting results on penile curvature and erectile function.
Several nondrug treatments for Peyronie's disease are being investigated, but evidence is limited on how well they work and possible side effects. These include using intense sound waves to break up scar tissue (shock wave therapy), stem cells, platelet-rich plasma and radiation therapy.
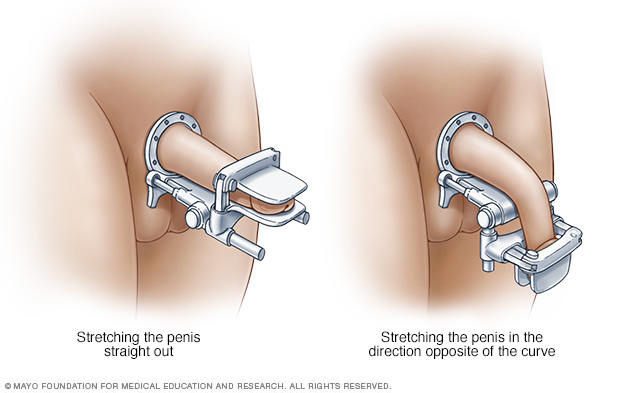
With penile traction therapy, you wear a penile traction device for a set amount of time each day. The device may stretch the penis straight out, or it may stretch the penis in the direction that's opposite of the curve.
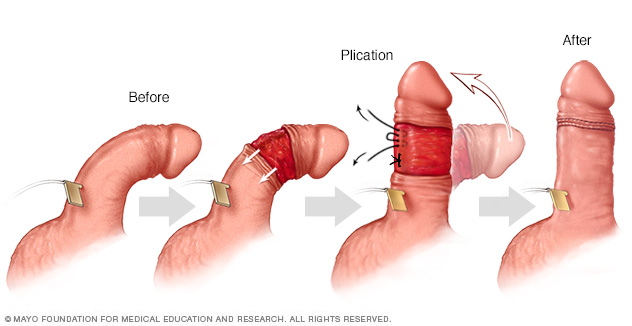
During plication of the penis, an artificial erection is created from either injection of a saltwater solution or selected medications. The outer skin of the penis is pulled back. The penis is straightened, and the excess tissue on what had been the outer side of the curve is cinched together by placing a series of stitches or "tucks." The final penile length will depend on the length of the shorter side — the side with the scarring from Peyronie's disease.
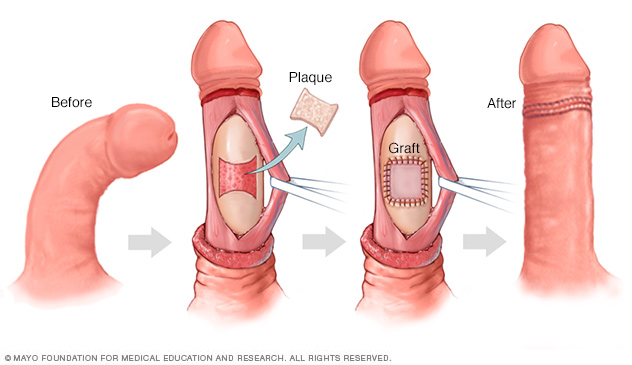
During a graft repair procedure, your surgeon makes one or more cuts (incisions) in the scar tissue (plaque) of the penis, allowing the sheath to stretch out and the penis to straighten. A patch made of human or animal tissue or a synthetic material is placed to cover the defect.
Coping and support
Peyronie's disease can be a source of significant anxiety and create stress between you and your sexual partner.
Here are some tips for coping with Peyronie's disease:
- Explain to your partner what Peyronie's disease is and how it affects your ability to have sex.
- Let your partner know how you feel about the appearance of your penis and your ability to have sex.
- Talk to your partner about how the two of you can maintain sexual and physical intimacy.
- Talk to a mental health provider who specializes in family relations and sexual matters.
Preparing for an appointment
If you have Peyronie's disease symptoms, you're likely to begin by seeing your family doctor or general practitioner. You might be referred to a specialist in male sexual disorders (urologist). If it's possible, encourage your partner to attend the appointment with you.
Preparing for your appointment will help you make the best use of your time.
What you can do
Make a list ahead of time that you can share with your doctor. Your list should include:
- Symptoms you're experiencing, including any that might seem unrelated to Peyronie's disease
- Key personal information, including any major stresses or recent life changes
- Medications that you're taking, including any vitamins or supplements
- History of injury to the penis
- Family history of Peyronie's disease, if any
- Questions to ask your doctor
List questions for your doctor from most important to least important in case time runs out. You might want to ask some of the following questions:
- What tests will I need?
- What treatment do you recommend?
- Can you tell if symptoms are likely to worsen or improve?
- Are there any brochures or other printed material that I can take home with me? What websites do you recommend?
In addition to the questions you've prepared to ask your doctor, don't hesitate to ask questions during your appointment.
What to expect from your doctor
Your doctor is likely to ask you a number of questions. Being ready to answer them might reserve time to go over any points you want to discuss further. Your doctor might ask:
- When did you first notice a curve in your penis or scar tissue under the skin of your penis?
- Has the curvature of your penis worsened over time?
- Do you have pain during erections, and if so, has it gotten worse or improved over time?
- Do you recall having an injury to your penis?
- Do your symptoms limit your ability to have sex?
Your doctor might also ask you to complete a survey, such as the International Index of Erectile Function, to help identify how the condition affects your ability to have sex.
Copyright © 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.