Premature ejaculation occurs in men when semen leave the body (ejaculate) sooner than wanted during sex. Premature ejaculation is a common sexual complaint. As many as 1 out of 3 people say they have it at some time.
Premature ejaculation isn't cause for concern if it doesn't happen often. But you might be diagnosed with premature ejaculation if you:
- Always or nearly always ejaculate within 1 to 3 minutes of penetration
- Are not able to delay ejaculation during sex all or nearly all the time
- Feel distressed and frustrated, and tend to avoid sexual intimacy as a result
Premature ejaculation is a treatable condition. Medications, counseling and techniques that delay ejaculation can help improve sex for you and your partner.
Symptoms
The main symptom of premature ejaculation is not being able to delay ejaculation for more than three minutes after penetration. But it might occur in all sexual situations, even during masturbation.
Premature ejaculation can be classified as:
- Lifelong. Lifelong premature ejaculation occurs all or nearly all the time beginning with the first sexual encounter.
- Acquired. Acquired premature ejaculation develops after having previous sexual experiences without problems with ejaculation.
Many people feel that they have symptoms of premature ejaculation, but the symptoms don't meet the criteria for a diagnosis. It's typical to experience early ejaculation at times.
When to see a doctor
Talk with your health care provider if you ejaculate sooner than you wish during most sexual encounters. It's common to feel embarrassed about discussing sexual health concerns. But don't let that keep you from talking to your provider. Premature ejaculation is common and treatable.
A conversation with a care provider might help lessen concerns. For example, it might be reassuring to hear that it's typical to experience premature ejaculation from time to time. It may also help to know that the average time from the beginning of intercourse to ejaculation is about five minutes.
Causes
The exact cause of premature ejaculation isn't known. It was once thought to be only psychological. But health care providers now know that premature ejaculation involves a complex interaction of psychological and biological factors.
Psychological causes
Psychological factors that might play a role include:
- Early sexual experiences
- Sexual abuse
- Poor body image
- Depression
- Worrying about premature ejaculation
- Guilty feelings that can cause you to rush through sex
Other factors that can play a role include:
- Erectile dysfunction. Being anxious about getting and keeping an erection might form a pattern of rushing to ejaculate. The pattern can be difficult to change.
- Anxiety. It's common for premature ejaculation and anxiety to occur together. The anxiety may be about sexual performance or related to other issues.
- Relationship problems. Relationship issues can contribute to premature ejaculation. This may be true if you've had sexual relationships with other partners in which premature ejaculation didn't happen often.
Biological causes
A number of biological factors might contribute to premature ejaculation. They may include:
- Irregular hormone levels
- Irregular levels of brain chemicals
- Swelling and infection of the prostate or urethra
- Inherited traits
Risk factors
Various factors can increase the risk of premature ejaculation. They may include:
- Erectile dysfunction. You might be at increased risk of premature ejaculation if you have trouble getting or keeping an erection. Fear of losing an erection might cause you to hurry through sex. This may happen whether you're aware of it or not.
- Stress. Emotional or mental strain in any area of life can play a role in premature ejaculation. Stress can limit the ability to relax and focus during sex.
Complications
Premature ejaculation can cause issues in your personal life. They might include:
- Stress and relationship problems. A common complication of premature ejaculation is relationship stress.
- Fertility problems. Premature ejaculation can sometimes make it hard for a partner to get pregnant. This may happen if ejaculation doesn't occur in the vagina.
Diagnosis
Your health care provider asks about your sex life and your health history. Your provider might also do a physical exam. If you have both early ejaculation and trouble getting or keeping an erection, your provider might order blood tests. The tests may check your hormone levels.
In some cases, your care provider might suggest that you go to a urologist or a mental health provider who specializes in sexual problems.
Treatment
Common treatment options for premature ejaculation include behavioral techniques, medications and counseling. It might take time to find the treatment or combination of treatments that work for you. Behavioral treatment plus drug therapy might be the most effective.
Behavioral techniques
In some cases, therapy for premature ejaculation involves simple steps. They may include masturbating an hour or two before intercourse. This may allow you to delay ejaculation when you have sex with your partner.
Your care provider might recommend avoiding intercourse for a period of time. Focusing on other types of sexual play may remove the pressure you might feel during sexual intercourse.
Pelvic floor exercises
Weak pelvic floor muscles might make it harder to delay ejaculation. Pelvic floor exercises (Kegel exercises) can help strengthen these muscles.
To perform these exercises:
- Find the right muscles. To find your pelvic floor muscles, stop urinating in midstream. Or tighten the muscles that keep you from passing gas. Both actions use your pelvic floor muscles. Once you've identified your pelvic floor muscles, you can exercise them in any position. However, you might find it easier to do them lying down at first.
- Perfect your technique. Tighten your pelvic floor muscles, hold for three seconds and then relax for three seconds. Try it a few times in a row. When your muscles get stronger, try doing Kegel exercises while sitting, standing or walking.
- Stay focused. For best results, focus on tightening only your pelvic floor muscles. Be careful not to flex the muscles in your abdomen, thighs or buttocks. Avoid holding your breath. Instead, breathe freely during the exercises.
- Repeat three times a day. Aim to do at least three sets of 10 repetitions a day.
The pause-squeeze technique
Your health care provider might instruct you and your partner to use the pause-squeeze technique. This method works as follows:
- Begin sexual activity, including stimulating the penis, until you feel almost ready to ejaculate.
- Then you or your partner can squeeze the end of your penis where the head joins the shaft. Keep squeezing for several seconds until the urge to ejaculate passes.
- Repeat the squeeze process as needed.
By repeating as many times as needed, you can reach the point of entering your partner without ejaculating. After some practice, delaying ejaculation might become a habit that no longer requires the pause-squeeze technique.
If the pause-squeeze technique causes pain or discomfort, you can try the stop-start technique. It involves stopping sexual stimulation just before ejaculation. Then waiting until the level of arousal has diminished and starting again.
Condoms
Condoms might make the penis less sensitive, which can help delay ejaculation. Specially designed "climax control" condoms are available without a prescription. These condoms contain numbing agents such as benzocaine or lidocaine to delay ejaculation. They might also be made of thicker latex. Examples include Trojan Extended Pleasure and Durex Prolong.
Medications
Topical numbing agents
Creams, gels and sprays that contain a numbing agent — such as benzocaine, lidocaine or prilocaine — are sometimes used to treat premature ejaculation. They're applied to the penis 10 to 15 minutes before sex to reduce sensation and help delay ejaculation. They're available without a prescription. However, a cream containing both lidocaine and prilocaine (EMLA) is available by prescription.
Although topical numbing agents are effective and well tolerated, they have potential side effects. They may cause decreased feeling and sexual pleasure in both partners.
Oral medications
Many medications might delay orgasm. These drugs aren't approved by the Food and Drug Administration to treat premature ejaculation, but some are used for this purpose. They include antidepressants, pain relievers and drugs for erectile dysfunction.
These medications might be prescribed for either on-demand or daily use. Also, they may be prescribed alone or with other treatments.
-
Antidepressants. A side effect of certain antidepressants is delayed orgasm. For this reason, selective serotonin reuptake inhibitors (SSRIs) are used to treat premature ejaculation. SSRIs include paroxetine (Paxil, Pexeva, Brisdelle), escitalopram (Lexapro), citalopram (Celexa), sertraline (Zoloft) or fluoxetine (Prozac).
The SSRI dapoxetine is often used as the first treatment for premature ejaculation in some countries. It's not currently available in the United States.
Of the drugs approved for use in the United States, paroxetine seems to be the most effective. These medications usually take 5 to 10 days to begin working. But it might take 2 to 3 weeks of treatment to see the full effect.
If SSRIs don't improve the timing of your ejaculation, your health care provider might prescribe the tricyclic antidepressant clomipramine (Anafranil). Side effects of antidepressants might include nausea, perspiration, drowsiness and decreased sex drive.
-
Pain relievers. Tramadol (Ultram, Conzip, Qdolo) is a medication used to treat pain. It also has side effects that delay ejaculation. Tramadol might be prescribed when SSRIs haven't been effective. Tramadol can't be used in combination with an SSRI.
Side effects might include nausea, headache, sleepiness and dizziness. Tramadol can become habit-forming when taken long-term.
- Phosphodiesterase-5 inhibitors. Some medications used to treat erectile dysfunction also might help premature ejaculation. These drugs include sildenafil (Viagra), tadalafil (Cialis, Adcirca), avanafil (Stendra) and vardenafil. Side effects might include headache, facial flushing and indigestion. These medications might be more effective when used in combination with an SSRI.
Potential future treatment
Research suggests that several drugs might be helpful in treating premature ejaculation. But more study is needed. These drugs include:
- Modafinil (Provigil). This is a treatment for the sleeping disorder narcolepsy.
- Silodosin (Rapaflo). This drug treats prostate gland enlargement.
- OnabotulinumtoxinA (Botox). Researchers are studying whether injecting Botox into the muscles that help cause ejaculation can treat premature ejaculation.
Counseling
This approach involves talking with a mental health provider about your relationships and experiences. Sessions can help you reduce performance anxiety and find better ways of coping with stress. Counseling is most likely to help when it's used in combination with drug therapy.
With premature ejaculation, you might feel that you lose some of the closeness shared with a sexual partner. You might feel angry, ashamed and upset, and turn away from your partner.
Your partner also might be upset with the change in sexual intimacy. Premature ejaculation can cause partners to feel less connected or hurt. Talking about the problem is an important step. Relationship counseling or sex therapy also might be helpful.
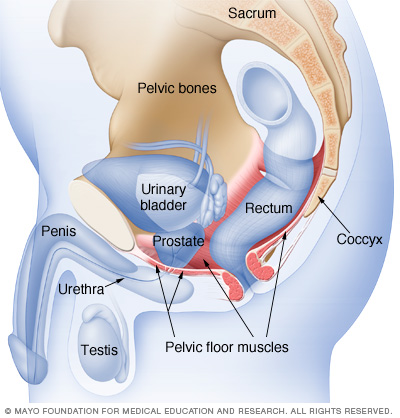
The pelvic floor muscles support the bladder and bowel and affect sexual function. Kegel exercises can help strengthen these muscles.
Alternative medicine
Several alternative medicine treatments have been studied, including yoga, meditation and acupuncture. However, more research is needed to determine their effectiveness.
Preparing for an appointment
It's typical to feel embarrassed when talking about sexual problems. But you can trust that your health care provider has had similar conversations with many others. Premature ejaculation is a very common condition. And it's one that can be treated.
Being ready to talk about premature ejaculation will help you get the treatment you need to put your sex life back on track. The information below should help you prepare to make the most of your appointment.
Information to gather in advance
- Pre-appointment restrictions. When you make your appointment, ask if there are any restrictions you need to follow in the time leading up to your visit.
- Symptoms. How often do you ejaculate before you or your partner would wish? How long after you begin having intercourse do you typically ejaculate?
- Sexual history. Think back on your relationships and sexual encounters since you became sexually active. Have you had problems with premature ejaculation before? With whom, and under what circumstances?
- Medical history. Write down any other medical conditions with which you've been diagnosed, including mental health conditions. Also note the names and strengths of all medications you are currently taking or have recently taken, including prescription drugs and those you buy without a prescription.
- Questions to ask your health care provider. Write down questions in advance to make the most of your time with your provider.
Basic questions to ask your doctor
The list below suggests questions to ask your health care provider about premature ejaculation. Don't hesitate to ask more questions during your appointment.
- What may be causing my premature ejaculation?
- What tests do you recommend?
- What treatment approach do you recommend?
- How soon after I begin treatment can I expect improvement?
- How much improvement can I reasonably expect?
- Am I at risk of this problem recurring?
- Is there a generic alternative to the medicine you're prescribing?
- Are there any brochures or other printed material that I can take home with me? What websites do you recommend visiting?
What to expect from your doctor
Your health care provider might ask very personal questions and might also want to talk to your partner. To help your provider determine the cause of your problem and the best course of treatment, be ready to answer questions, such as:
- How often do you have premature ejaculation?
- When did you first experience premature ejaculation?
- Do you have premature ejaculation only with a specific partner or partners?
- Do you experience premature ejaculation when you masturbate?
- Do you have premature ejaculation every time you have sex?
- How often do you have sex?
- How much are you bothered by premature ejaculation?
- How much is your partner bothered by premature ejaculation?
- How satisfied are you with your current relationship?
- Are you also having trouble getting and keeping an erection (erectile dysfunction)?
- Do you take prescription medications? If so, what medications have you recently started or stopped taking?
- Do you use recreational drugs?
What you can do in the meantime
Deciding to talk with your health care provider is an important step. In the meantime, consider exploring other ways in which you and your partner can connect. Although premature ejaculation can cause strain and anxiety in a relationship, it is a treatable condition.
Copyright © 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.