Solitary rectal ulcer syndrome is a condition that occurs when one or more open sores (ulcers) develop in the rectum. The rectum is a muscular tube connected to the end of your colon. Stool passes through the rectum on its way out of the body.
Solitary rectal ulcer syndrome is a rare and poorly understood disorder that often occurs in people with chronic constipation. Solitary rectal ulcer syndrome can cause rectal bleeding and straining during bowel movements. Despite the name, sometimes more than one rectal ulcer occurs in solitary rectal ulcer syndrome.
Solitary rectal ulcer syndrome may improve with simple lifestyle strategies, such as changing your diet and drinking more fluids. In severe cases, however, surgery may be needed.
Symptoms
Signs and symptoms of solitary rectal ulcer syndrome include:
- Constipation
- Rectal bleeding
- Straining during bowel movements
- Pain or a feeling of fullness in your pelvis
- A feeling of incomplete passing of stool
- Passing mucus from your rectum
- Fecal incontinence
- Rectal pain
However, some people with solitary rectal ulcer syndrome may experience no symptoms.
When to see a doctor
Make an appointment with your doctor if you notice any signs or symptoms that worry you.
Several other conditions may cause signs and symptoms similar to those of solitary rectal ulcer syndrome. At your appointment, your doctor may recommend tests and procedures to identify or rule out causes other than solitary rectal ulcer syndrome.
Causes
It's not always clear what causes solitary rectal ulcer syndrome. Doctors believe stress or injury to the rectum may cause rectal ulcers to form.
Among the things that could injure the rectum are:
- Constipation or hardened stool in the rectum that's difficult to pass (impacted stool)
- Straining during bowel movements
- A stretched rectum that comes out of the anus (rectal prolapse)
- Uncoordinated tightening of the pelvic floor muscles that slows blood flow to the rectum
- Attempts to manually remove impacted stool
- When one part of the intestine slides inside another part (intussusception)
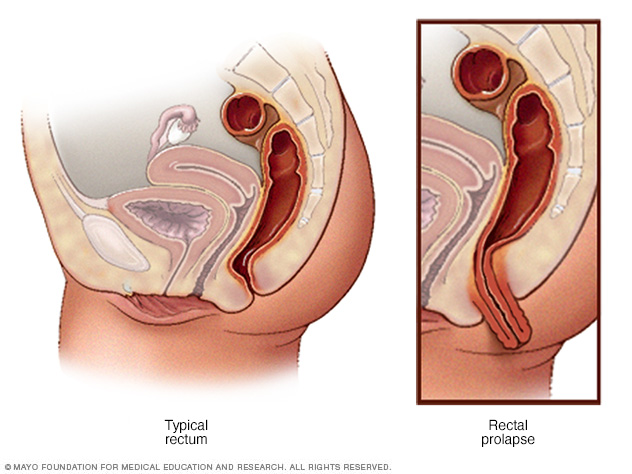
Rectal prolapse occurs when the rectum becomes stretched out and protrudes from the anus.
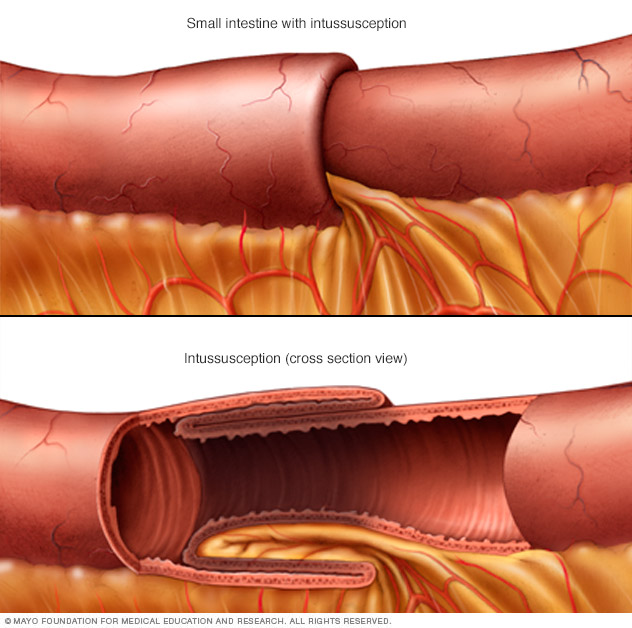
Intussusception is a rare, serious disorder in which one part of the intestine slides inside an adjacent part.
Diagnosis
You may have one or more of the following tests to diagnose solitary rectal ulcer syndrome:
- Sigmoidoscopy. During this test, your doctor inserts a thin, flexible tube with a tiny camera into your rectum to examine your rectum and part of your colon. If a lesion is found, your doctor may take a tissue sample for laboratory testing.
- Ultrasound. This imaging technique uses sound waves to create pictures. Your doctor may recommend an ultrasound to help differentiate solitary rectal ulcer syndrome from other conditions.
-
Other imaging studies. Your doctor may order an imaging study called defecation proctography. In this study, a soft paste made of barium is inserted into your rectum. You then pass the barium paste as you would stool. The barium shows up on X-rays and may reveal a prolapse or problems with muscle function and muscle coordination.
Specialized centers may offer a similar test called magnetic resonance defecography. This test is done with a magnetic resonance imaging machine and provides a 3D image of the rectum.
Treatment
Treatment for solitary rectal ulcer syndrome depends on the severity of your condition. People with mild signs and symptoms may find relief through lifestyle changes, while people with more severe signs and symptoms may require medical or surgical treatment.
- Dietary changes. To relieve constipation, you may be given tips on increasing fiber in your diet.
-
Behavior therapy. You may strain during bowel movements out of habit. Behavior therapy can help you learn to relax your pelvic muscles during bowel movements.
In one behavioral technique, called biofeedback, a specialist teaches you to control certain involuntary body responses, such as the tightening of your anus or pelvic floor muscles, during defecation. Biofeedback may make you more aware of your straining and help you to control it.
- Medications. Certain treatments such as topical steroids, sulfasalazine enemas and onabotulinumtoxinA (Botox) may help ease your rectal ulcer symptoms. However, these treatments don't work for everyone, and some are still considered experimental.
Surgical procedures used to treat solitary rectal ulcer syndrome include:
- Rectal prolapse surgery. If you have a rectal prolapse that's causing symptoms, your doctor may recommend a rectopexy procedure. Rectopexy secures the rectum in its anatomically correct position.
- Surgery to remove the rectum. An operation to remove the rectum may be an option if you have severe signs and symptoms that haven't been helped by other treatments. The surgeon may connect the colon to an opening in the abdomen for waste to leave the body (colostomy). If you have a colostomy, a pouch or bag is then attached to your abdomen to collect waste.
Lifestyle and home remedies
You can make changes to your daily life that may help relieve your symptoms. Such changes are likely to include:
-
Increasing the amount of fiber in your diet. Fiber adds bulk to your stool. The bulk helps push the contents of your intestines along so that they can be eliminated when you have a bowel movement. Aim for 14 grams of fiber for every 1,000 calories in your daily diet.
Nutrition labels on food packaging list the amount of fiber in a serving. The best sources of fiber are fruits, vegetables and whole grains. Eat fruits and vegetables with the skin on, and choose whole fruits and vegetables over juices. Look for breads and cereals that list whole wheat, oats or bran as the first ingredients.
-
Trying bulk laxatives and stool softeners. Bulk laxatives, such as psyllium husk (Metamucil, Natural Fiber Therapy, others) and calcium polycarbophil (FiberCon, Fiber-Lax, others), absorb fluid in the intestines and make stools bulkier, which helps trigger the bowel to contract and push stool out. However, they should be taken with water or they can cause obstruction.
Stool softeners, such as docusate (Colace, Surfak, others), help mix fluid into stools, making them easier to pass.
- Drinking water throughout the day. Drinking enough water and other fluids helps to keep your bowel movements soft and easy to pass. For variety, you may want to add lemon juice to water for flavor. Or try other noncarbonated and caffeine-free beverages. Prune juice can be helpful because it has a natural laxative effect.
Preparing for an appointment
Start by seeing your primary doctor if you have signs or symptoms that worry you. If your doctor suspects that you may have solitary rectal ulcer syndrome, you may be referred to a doctor who specializes in the digestive system (gastroenterologist).
What you can do
- Be aware of any pre-appointment restrictions. At the time you make the appointment, be sure to ask if there's anything you need to do in advance, such as restrict your diet.
- Write down key personal information, including any major stresses or recent life changes.
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Make a list of all medications, vitamins or supplements that you're taking.
- Write down questions to ask your doctor.
For solitary rectal ulcer syndrome, some basic questions to ask your doctor include:
- What is likely causing my rectal ulcer signs and symptoms?
- What are other possible causes for my symptoms?
- What kinds of tests do I need?
- Is my condition likely temporary or long lasting?
- Do I need treatment?
- What are my treatment options?
- How can I best manage other conditions I have while being treated for this condition?
- Do I need to follow any dietary or activity restrictions?
- Is there a generic alternative to the medicine you're prescribing me?
- Are there any brochures or other printed material that I can take with me?
- What websites do you recommend?
- Will I need follow-up visits? If so, how often?
What to expect from your doctor
Your doctor is likely to ask you a number of questions. If you've thought about your answers, you may have additional time to go over any points you want to spend more time on.
Your doctor may ask:
- When did you first begin having these symptoms?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- Have you recently had trouble with constipation?
- Does anything seem to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
Copyright © 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.