Tricuspid atresia is a heart defect present at birth (congenital) in which a valve (tricuspid valve) between two of the heart's chambers isn't formed. Instead, there's solid tissue between the chambers, which restricts blood flow and causes the right lower heart chamber (ventricle) to be underdeveloped.
A baby, child or adult with tricuspid atresia can't get enough oxygen through its body. People with this condition tire easily, are often short of breath and have blue-tinged skin.
Tricuspid atresia is treated with multiple surgeries. Most babies with tricuspid atresia who have surgery live well into adulthood, though follow-up surgeries are often needed.
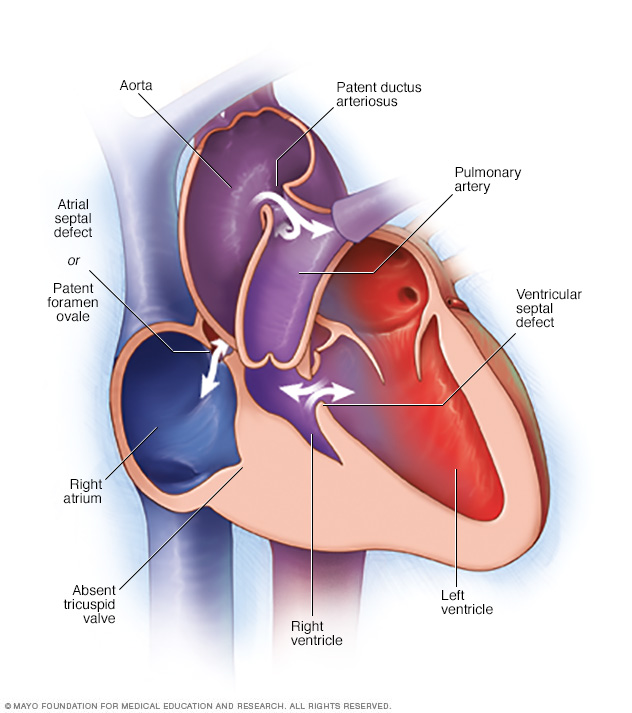
In tricuspid atresia, blood can't flow from the right atrium to the right ventricle because the valve between them is missing. This condition often includes a smaller than normal right ventricle, as well as an atrial septal defect and, in some cases, a ventricular septal defect.
Symptoms
Tricuspid atresia symptoms become evident soon after birth, and can include:
- Blue tinge to the skin and lips (cyanosis)
- Difficulty breathing
- Tiring easily, especially during feedings
- Slow growth and poor weight gain
Some babies or older people with tricuspid atresia also develop symptoms of heart failure, including:
- Fatigue and weakness
- Shortness of breath
- Swelling (edema) in the legs, ankles and feet
- Swelling of the abdomen (ascites)
- Sudden weight gain from fluid retention
When to see a doctor
Tell your doctor if you notice any of the above symptoms in yourself or your child.
Causes
Tricuspid atresia occurs during fetal heart development. Some genetic factors, such as Down syndrome, might increase your baby's risk of congenital heart defects such as tricuspid atresia, but the cause of congenital heart disease is usually unknown.
How the heart works
Your heart is divided into four chambers — the right atrium and right ventricle and left atrium and left ventricle. The right side of the heart moves blood to the lungs, where it picks up oxygen before it circulates to your heart's left side. The left side pumps blood into a large vessel called the aorta, which circulates the oxygen-rich blood to the rest of your body.
Valves control the flow of blood into and out of your heart. These valves open to allow blood to move to the next chamber or one of the arteries, and they close to keep blood from flowing backward.
When things go wrong
In tricuspid atresia, the right side of the heart can't pump enough blood to the lungs because the tricuspid valve is missing. A sheet of tissue blocks the flow of blood from the right atrium to the right ventricle. As a result, the right ventricle is usually small and underdeveloped (hypoplastic).
Blood instead flows from the right atrium to the left atrium through a hole in the wall between them (septum). This hole is either a heart defect (atrial septal defect) or an enlarged natural opening that's supposed to close soon after birth (patent foramen ovale).
After the blood flows to the left atrium, it enters the left ventricle and then is pumped to the aorta. To get to the lungs, blood flows through a vessel that connects the aorta to the pulmonary artery (ductus arteriosus). All hearts have a ductus arteriosus while the baby is in the uterus, but shortly after birth, the ductus closes.
A baby with tricuspid atresia might need medication to keep the ductus from closing after birth. A procedure or surgery to create an opening between the atria or to provide a connection from the aorta to the pulmonary artery might be needed.
Many babies born with tricuspid atresia have a hole between the ventricles (ventricular septal defect). In these cases, some blood can flow through the hole between the left ventricle and the right ventricle, and then blood is pumped to the lungs through the pulmonary artery.
However, the valve between the right ventricle and the pulmonary artery (pulmonary valve) might be narrowed, which can reduce blood flow to the lungs. If the pulmonary valve isn't narrowed and if the ventricular septal defect is large, too much blood can flow to the lungs, which can lead to heart failure.
Some babies have other heart defects as well.

A typical heart has two upper and two lower chambers. The upper chambers, the right and left atria, receive incoming blood. The lower chambers, the more muscular right and left ventricles, pump blood out of the heart. The heart valves, which keep blood flowing in the right direction, are gates at the chamber openings.
Risk factors
In most cases, the cause of a congenital heart defect, such as tricuspid atresia, is unknown. However, several things might increase the risk of a baby being born with a congenital heart defect, including:
- A mother who had German measles (rubella) or another viral illness during early pregnancy
- A parent who has a congenital heart defect
- Drinking alcohol during pregnancy
- Smoking before or during pregnancy
- A mother who has poorly controlled diabetes
- Use of some types of medications during pregnancy, such as the acne drug isotretinoin (Claravis, Amnesteem, others), some anti-seizure medications and some bipolar disorder medications
- The baby is born with Down syndrome, a genetic condition that results from an extra 21st chromosome
Complications
A life-threatening complication of tricuspid atresia is a lack of oxygen to your baby's tissues (hypoxemia).
Complications later in life
Although treatment greatly improves the outcome for babies with tricuspid atresia, complications can develop later in life, including:
- Formation of blood clots that can lead to a clot blocking an artery in the lungs (pulmonary embolism) or cause a stroke
- Easy tiring when participating in activity or exercise
- Heart rhythm abnormalities (arrhythmias)
- Kidney or liver disease
Prevention
Congenital heart defects such as tricuspid atresia usually aren't preventable. If you have a family history of heart defects or a child with a congenital heart defect, a genetic counselor and a cardiologist experienced in congenital heart defects can help you look at risks associated with future pregnancies.
Some steps you can take that might reduce your baby's risk of heart and other birth defects in pregnancy include:
- Get adequate folic acid. Take 400 micrograms of folic acid daily. This amount, which is often in prenatal vitamins, has been shown to reduce brain and spinal cord defects, and folic acid may help prevent heart defects, too.
- Talk with your doctor about medication use. Whether you're taking prescription or over-the-counter drugs, an herbal product or a dietary supplement, check with your doctor before using them during pregnancy.
- Avoid smoking or drinking alcohol during pregnancy. Either can increase the risk of congenital heart defects.
- Avoid chemical exposure, whenever possible. While you're pregnant, it's best to stay away from chemicals, including cleaning products and paint, as much as you can.
Diagnosis
Before birth
Because of advances in ultrasound technology, doctors can usually identify tricuspid atresia on a routine ultrasound exam during gestation.
After birth
Your baby's doctor might suspect a heart defect, such as tricuspid atresia, if your newborn has blue-tinged skin or is having trouble breathing.
Another indication is hearing an abnormal whooshing sound caused by blood not flowing properly (heart murmur), when listening to your baby's heart during a physical exam.
If tricuspid atresia is suspected, your baby's doctor might order tests including:
- Echocardiogram. This test uses sound waves that bounce off your baby's heart to produce moving images the doctor can view on a video screen. In a baby with tricuspid atresia, the echocardiogram reveals the absence of a tricuspid valve, irregular blood flow and other heart defects.
- Electrocardiogram (ECG). This test records the electrical activity of the heart and can determine whether the heart's chambers are enlarged, or the heart rhythm is abnormal.
- Pulse oximetry. This measures the oxygen in your or your baby's blood using a sensor placed over the end of your or your baby's finger.
- Chest X-ray. This might show whether the heart and its chambers are enlarged. It can also show whether there is too much or too little blood flow to the lungs.
- Cardiac catheterization. A thin, flexible tube (catheter) is inserted into a blood vessel at your child's groin and guided into the heart. Rarely used to diagnose tricuspid atresia, this test might be used to examine the heart before surgery to treat tricuspid atresia.
Treatment
There's no way to replace a tricuspid valve in tricuspid atresia. Treatment involves surgery to ensure enough blood flow through the heart and into the lungs.
Often, this requires more than one surgery. Medications to strengthen the heart muscle, lower blood pressure and rid the baby's body of excess fluid and supplemental oxygen to help the baby breathe also might be given before surgery.
Medications
Before surgery, your child's cardiologist might recommend that your child take the hormone prostaglandin to help widen (dilate) and keep open the ductus arteriosus.
Surgeries or other procedures
Some of the procedures used to treat tricuspid atresia are a temporary fix to increase blood flow (palliative surgeries). Procedures that might be needed include:
- Atrial septostomy. Rarely, a balloon is used to create or enlarge the opening between the heart's upper chambers to allow more blood to flow from the right atrium to the left atrium.
-
Shunting. This creates a bypass (shunt) from a main blood vessel leading out of the heart to the blood vessel leading to the lungs (pulmonary artery), which improves oxygen levels.
Surgeons generally implant a shunt during the first two weeks of life. However, babies usually outgrow this shunt and might need another surgery to replace it.
- Pulmonary artery band placement. If your baby has a ventricular septal defect and too much blood flowing to the lungs from the heart, a surgeon might place a band around the pulmonary artery to reduce the flow.
-
Glenn operation. When babies outgrow the first shunt, they often require this surgery, which sets the stage for the more permanent corrective surgery, called the Fontan procedure.
Doctors usually perform the Glenn operation when a child is between 3 and 6 months old. Doctors remove the first shunt, then connect one of the large veins that normally returns blood to the heart (the superior vena cava) to the pulmonary artery instead.
This procedure allows blood to flow directly to the lungs and reduces the workload on the left ventricle, decreasing the risk of damage to it.
-
Fontan procedure. A variation of this standard treatment of tricuspid atresia is usually done when the child is 2 to 5 years old. In general, the surgeon creates a path for the blood that's returning to the heart (the inferior vena cava) to flow directly into the pulmonary arteries, which then transport the blood into the lungs.
Doctors sometimes leave an opening between the pathway and the right atrium (fenestration).
Follow-up care
To monitor heart health, you or your child will need lifelong follow-up care with a cardiologist who specializes in congenital heart disease.
Your or your child's cardiologist will tell you whether you or your child needs to take preventive antibiotics before dental and other procedures. In some cases, your child's cardiologist might recommend limiting vigorous physical activity.
The short- and intermediate-term outlook for children who have a Fontan procedure is generally promising. A variety of complications can occur over time and require additional monitoring and procedures.
Failure of the circulation system created by the Fontan procedure might make a heart transplant necessary.
Lifestyle and home remedies
Here are some tips for caring for your child with tricuspid atresia:
-
Strive for good nutrition. Your baby might not be getting enough calories because of tiring during feeding and an increased need for calories. It's often helpful to give your baby frequent, small feedings.
Breast milk is an excellent source of nutrition, but if your baby isn't getting enough nutrition because of tiring during feeding, your doctor might prescribe a special high-calorie formula. Some babies might need to be fed through a feeding tube.
-
Preventive antibiotics. Your or your child's cardiologist will likely recommend preventive antibiotics be taken before certain dental and other procedures to prevent bacteria from infecting the inner lining of the heart (infective endocarditis).
Practicing good oral hygiene — brushing and flossing teeth, getting regular dental checkups — also helps prevent infection.
- Stay active. Encourage as much normal play and activity as you or your child can tolerate or as your doctor recommends, with ample opportunity for rest. Staying active helps your or your child's heart stay fit.
- Keep up with routine medical and well-child care. Standard immunizations are encouraged for children with congenital heart defects, as well as vaccines against the flu, pneumonia and respiratory syncytial virus infections. Your child should take all medications as prescribed.
- Keep follow-up appointments with your or your child's doctor. Your child will need at least annual appointments with a doctor trained in congenital heart conditions. Your child's doctor is likely to recommend several tests to evaluate your or your child's heart condition.
Adults with tricuspid atresia
If you're an adult with tricuspid atresia, you need to be seen regularly throughout your life by a doctor trained in adult congenital heart conditions. Your doctor is likely to recommend regular tests to evaluate your condition at these appointments.
Your doctor might recommend that you take preventive antibiotics before certain dental or medical procedures to prevent infective endocarditis.
Ask your doctor about what activities are best for you, and if there are sports or activities that you should limit or avoid.
Tricuspid atresia and pregnancy
Women with tricuspid atresia who are considering pregnancy should talk to a doctor who specializes in adult congenital heart diseases as well as a maternal-fetal medicine specialist. If you do become pregnant, it's best to see a doctor who specializes in pregnancies in women with congenital heart disease.
For women who have had a Fontan procedure, pregnancy will be considered high-risk. Some women, such as those with a history of heart failure, will be discouraged from becoming pregnant.
Coping and support
Caring for a baby with a serious heart problem such as tricuspid atresia can be challenging. Here are some strategies that might help:
- Try to maintain normalcy and closeness. Maintaining a regular daily routine will help both you and your child. Even if your baby is in the hospital, try to spend as much time together as you can. Include other children you have. Family bonding is important for your baby's social and emotional development.
- Seek support. Ask family members and friends for help. Ask your child's cardiologist about support groups and other types of assistance. The American Heart Association offers a support group called Mended Little Hearts.
- Record your baby's health history. Write down your baby's diagnosis, medications, surgery and other procedures and their dates, the name and phone number of your child's cardiologist, and other important information about your baby's care. It's also helpful to keep copies of surgical reports.
- Talk about your concerns. As your child grows and develops, discuss your concerns about his or her health with your child's cardiologist.
Remember that many children with congenital heart defects, such as tricuspid atresia, grow up to lead full lives.
Preparing for an appointment
Eventually you or your baby will see a cardiologist with experience in treating congenital heart defects. Here's some information to help you get ready for the appointment.
What you can do
Make a list of:
- Symptoms you've noticed in yourself or your child, including any that may seem unrelated to a heart defect
- Important personal information, including family history of congenital heart disease, illnesses the mother had during pregnancy or behaviors, such as smoking, during pregnancy
- Questions to ask your doctor
Take a family member or friend along, if possible, to help you remember the information your doctor gives you.
For a congenital heart defect, questions to ask the cardiologist include:
- What tests are needed?
- What treatments are available, and which do you recommend?
- Will this require more than one surgery?
- How can I make myself or my child more comfortable?
- Are there restrictions to follow?
- If I get pregnant again, is there a way to prevent this from happening again?
- Are there brochures or other printed material that I can have? What websites do you recommend?
Don't hesitate to ask other questions.
What to expect from your doctor
Your doctor is likely to ask you questions, such as:
- Have symptoms been continuous or occasional?
- What, if anything, seems to improve the symptoms?
- Does anything worsen the symptoms?
Copyright © 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.